Definition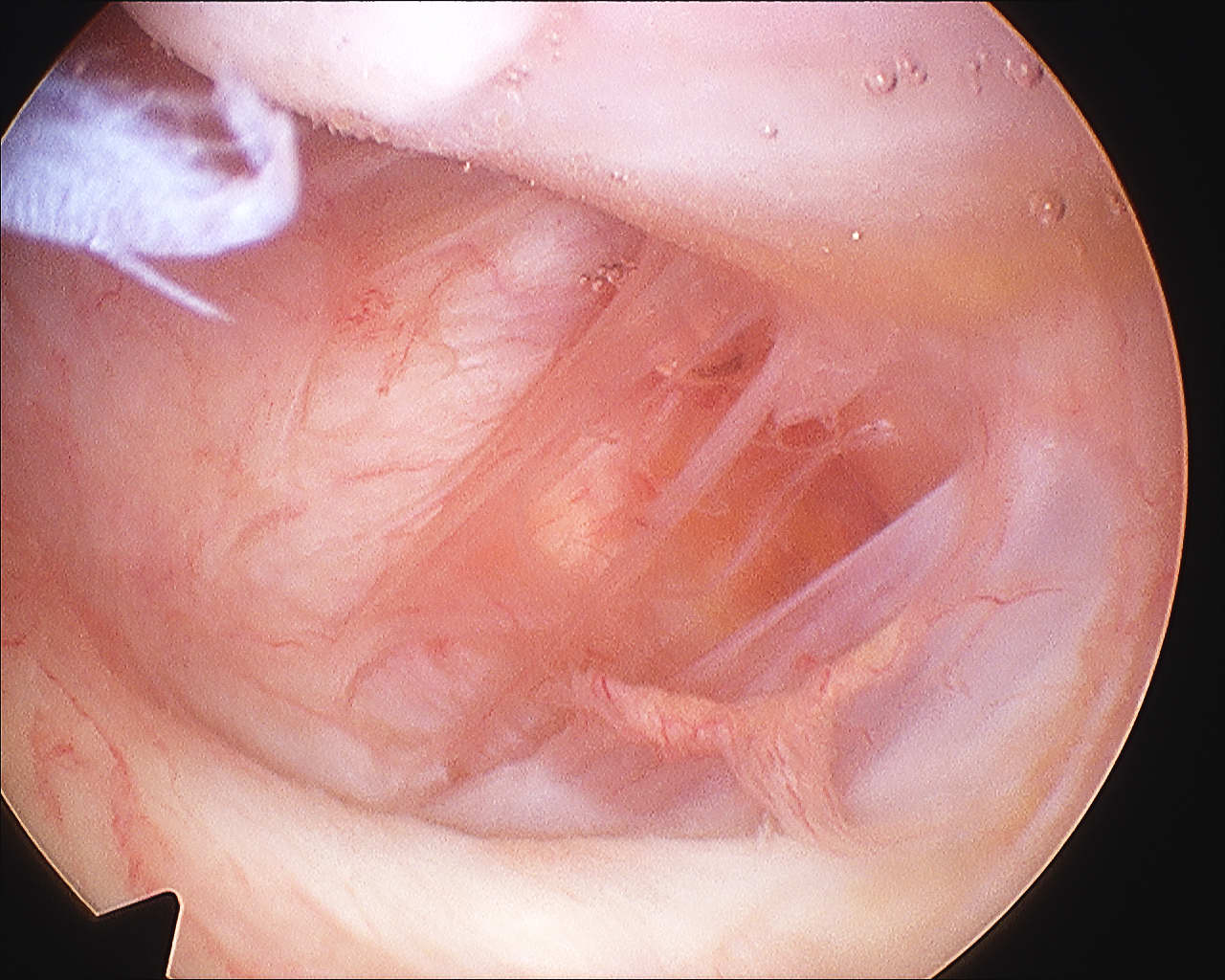
Humeral Avulsion of Glenohumeral Ligament
Incidence
Bokor et al JBJS Br 1999
- 514 cases surgical treatment traumatic instability
- incidence 7.5%
- 25% associated SSC tear
- likelihood of HAGL if no Bankart or MDI 27%
Bhatia KSSTA 2012
- 10% incidence of HAGL
Bigliani et al J Ortho Research 1992
- cadaveric dislocations
- 25% HAGL
Why the difference with cadavers
- ? differences in tissue
- HAGL lesions heal / don't always cause instability
Type
Bony avulsions (BHAGL)
Soft tissue
- humeral
- humeral and bankart (floating)
- posterior / Reverse HAGL
Pathology
Pouliart J Should Elbow Surg 2006
- cadaveric study
- extensive capsular injury +/- SSC required for HAGL to cause instability
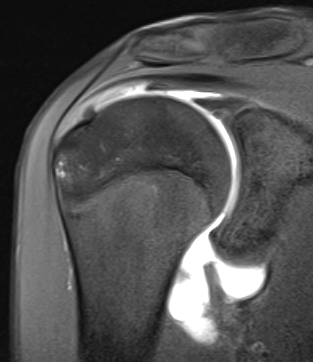
MRA
Normal
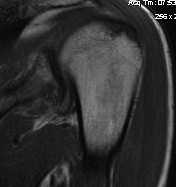

Abnormal
- J sign
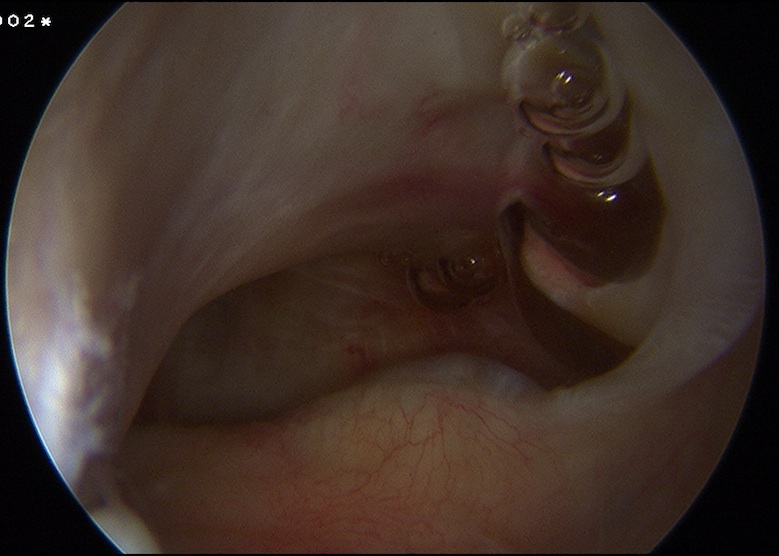
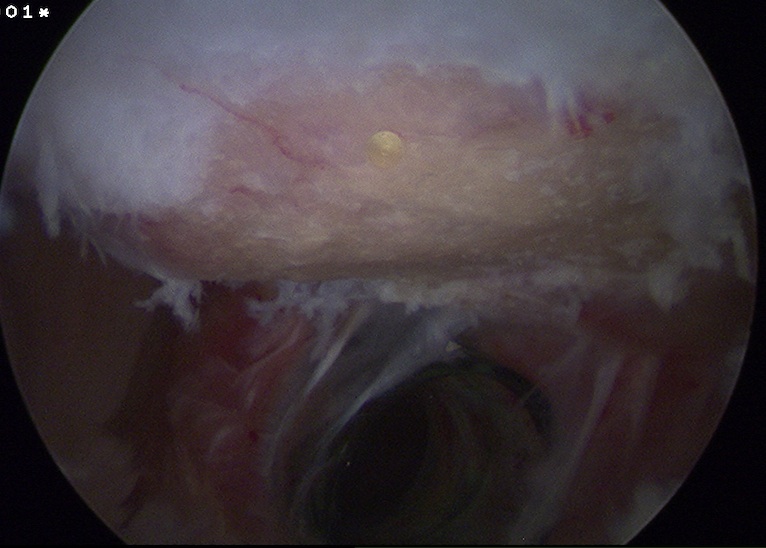
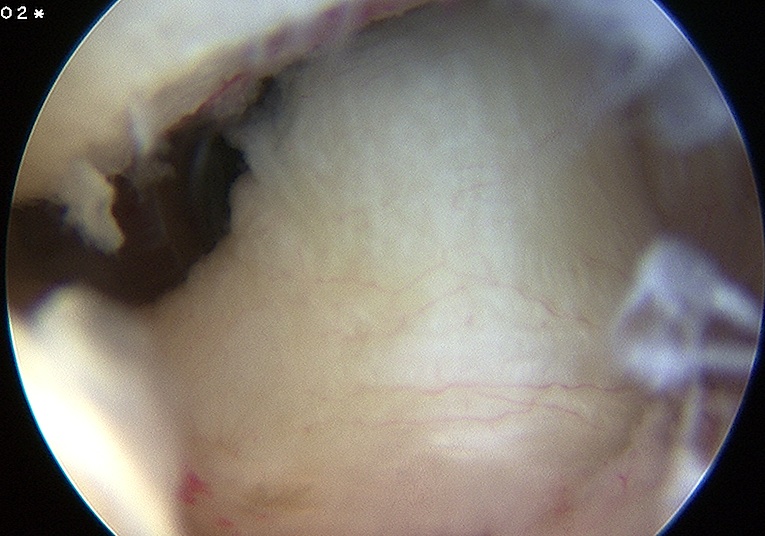
Arthroscopy
Normal
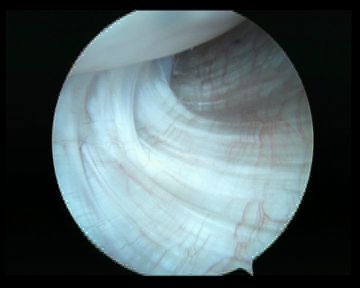
Abnormal
Management
1. HAGL
Open Technique
Detach lower half SSC
- L Shaped tenotomy
- repair IGHL to surgical NOH
Arthroscopic Technique
Burkhart
- 70o scope
- 5 o'clock portal through SSC with arm adducted
- danger to MCN if arm abducted at all with insertion 5 o'clock portal
- ensure good angle to proximal humerus with needle, for insertion of anchors
- may use suture passers from posterior portal
2. Bankart + HAGL (Floating)
Options
- arthroscopic repair both
- open repair both
- arthroscopic repair bankart, open HAGL
- arthroscopic repair bankart, leave HAGL
Kim et al Arthroscopy Supplement 2006
- all arthroscopic, 8 good results
Rhee et al J Should Elbow Surg 2007
- 4 floating HAGL, open treatment
- loss 15o ER
- elected to leave humeral side in volleyballer for risk of loss of ER
Bhatia KSSTA 2012
- subscap sparing approach in 7 patients
- good outcome