Definition
Lateral curvature of the spine with vertebral rotation
- defined as > 10o coronal plane deformity
- occurs at or near the onset of puberty
- no cause is established
Planes of Deformity
Triplanar
- coronal / scoliosis
- sagittal / thoracic lordosis
- transverse / rotational
General Categories
Structural
Fixed lateral curvature with rotational deformity
- intrinsic anatomical change
1. Idiopathic 75%
2. Neuromuscular 10%
3. Congenital 10%
4. Other 5%
Non structural
Reversible, non rotational and disappears with sitting
- nil intrinsic anatomical change
Compensatory / Hysterical / Irritative / Postural / Sciatic
Incidence
< 10o - 2.5 %
> 30o 4 / 1000
> 40o 1/1000
Gender
- little difference overall
- females more likely to have larger curves
- females more likely to progress
Classification
Scoliosis Research Society (SRS)
Infantile: 0-3 years onset
Juvenile: 3-10 (Puberty)
Adolescent: 10 - Cessation of Growth (20 years)
Alternative
Early Onset - < 5 years
- rare and severe
- male 2:1
- left sided
- if less than 1, 90% resolve
- >1, 20% resolve
- many other congenital anomalies
Late Onset - > 5 years
- Adolescent Idiopathic
- females 6:1
- right thoracic
- nil associations
- FHx common
Aetiology
Structural Differences
Intervertebral Disc
- decreased GAG in Nucleus and increased collagen content
Paravertebral Muscles
- differences in muscle fibres on either side of curve
- more type I fibres on the convex side of curve
Ligaments and Tendons
- PLL thickened
Endocrine
- patients with idiopathic scoliosis often taller
- normal GH but altered Somatomedin levels - ? significance
Vertebral Body
- structures on concave side hypoplastic
- structures on convex side hyperplastic
- due to persistent asymmetrical loading
Postural Equilibrium
- abnormality in vestibular system in brainstem
- scoliosis induced in bipedal rats with destruction of brainstem
- not conclusive - ? effect rather than cause
Neurotransmitter
Scoliosis produced when the pineal gland removed from chickens
- transmitter found to date - ? melatonin
Genetics
Increased incidence in affected relatives
Mother with scoliosis
- 10% chance for female child
Sister with scoliosis
- 20% chance for female child
Mother and father with scoliosis
- 80% chance for female child
Lordosis
Biomechanical initiator of the deformity
- thoracic lordosis normally lies in front of the normal axis of rotation
- causes the lumbar lordotic section to rotate in flexion
- the tethering of the posterior elements (thickened PLL) also contributes to rotation in flexion
- explains the Crank Shaft Phenomena
Adolescent Idiopathic Scoliosis
Epidemiology
Prevalence dependant on the size of the curve
As the curve increases in magnitude the female preponderance increases as well
Overall is 3.6:1 F:M
Curve Patterns
There are five major curve patterns in decreasing order they are
Right Thoracic
Double major (Thoracic dominant)
Thoracolumbar
Double major (Lumbar dominant)
Left Lumbar
Progression
Definition
Absolute increase in Cobb angle of 10o
- or 5o over two consecutive visits
Remember the interobserver error of Cobb angles is +/- 4o
- can vary with the time of day (increases in the pm)
Factors related to progression
MR Sex MAP
Magnitude: curve > 20o
Risser: 0 or 1
Sex: Female
Menarche: premenarche
Age: < 12
Pattern: Thoracic & double curves most
Growth Remaining
Menarche
- 66% prior to and 33% after menarche
- most growth is 1 year before and 1 year after menarche
- have on average 2 years growth left
- have passed PHV
PHV
- peak height velocity / most important factor
- adolescent growth spurt
- girls 8 cm / year
- boys 9.5 cm / year
- before menarche / at Risser 0 / open triradiate cartilage
- PHV generally over 2 years
Tanner sign
I - Pre-pubertal
II - Breast buds - related to adolescent growth spurt
III- Pubic hair
IV- Menarche
Triradiate cartilage
- may be more sensitive in judging the maturity
- Risser 0 + open triradiate cartilage indicates a lot of growth to go
- closes in the middle of the PHV
Risser sign
Risser grade relies on ossification of the iliac apophysis from lateral to medial and is completed with maturity
- Grade 0 to 5
- Grade 0 means no ossified apophysis present
- Grade 1 means appearance of apophysis laterally / after menarche
- Grade 5 is fusion of the apophyseal cap to ilium / little growth remaining / 14-16 Boys and 11-13 Girls
- can be difficult to distinguish between 0 and 5
Curve Pattern
Double curves have higher incidence of progression than single curves
- single thoracic > single lumbar
- lumbar the least
Curve Progression Studies
1. Lowenstein Study of Curve Progression
Looked at Risser sign + intial curve in regards to curve progression
| Risser | 0 - 1 | 2 - 5 | |
| Initial curve | 0 - 19o | 22% | 2% |
| Initial curve | 19 - 290 | 66% | 22% |
2. Weinstein and Ponsetti
Looked at the progression after maturity / 30 year study
- curves less than 30o as rule DO NOT progress after maturity
- 50 - 75o progressed most ( 1o/ year )
- this is the basis for surgery for curves 450 plus
Slowed over 100o with costopelvic impingement
Findings
- mortality 2x expected
- high percentage disability pension
- none in heavy work
- nil increase incidence LBP
Natural History of Untreated Scoliosis
Back Pain
Most studies suggest that the incidence of back pain is no higher than in general population
Back pain seen in thoracolumbar or lumbar curves of > 45o
- particularly if large apical rotation or imbalance
Pulmonary Function
Affect on pulmonary function not seen until curves of 80o reached
- restrictive pattern
- linear relationship between FVC and PaO2 and curve size
- nil effect with curve < 60o
- 1/3 with curve 60-100o
- 1/2 with curve > 100o
Mortality
Nachemson 1968
- not increased until curve of 100o noted
Cor Pulmonale
Seen at 40 and 50 years of age if curve > 80o
Assessment
History
How detected
Presence of progression
Associated complaints
- pain
- neurological symptoms
- respiratory symptoms
Status of growth
- growth spurt
- menarche
- changes in puberty
Want to ensure is idiopathic
- normal delivery / normal milestones
- bladder troubles (NM)
- Marfinoid / OI / NF
Examination
See the section on examination for detail
AP Film
Standing AP or PA films of whole spine including the iliac crests
- PA has less radiation to ovaries and breasts
- AP has less magnification
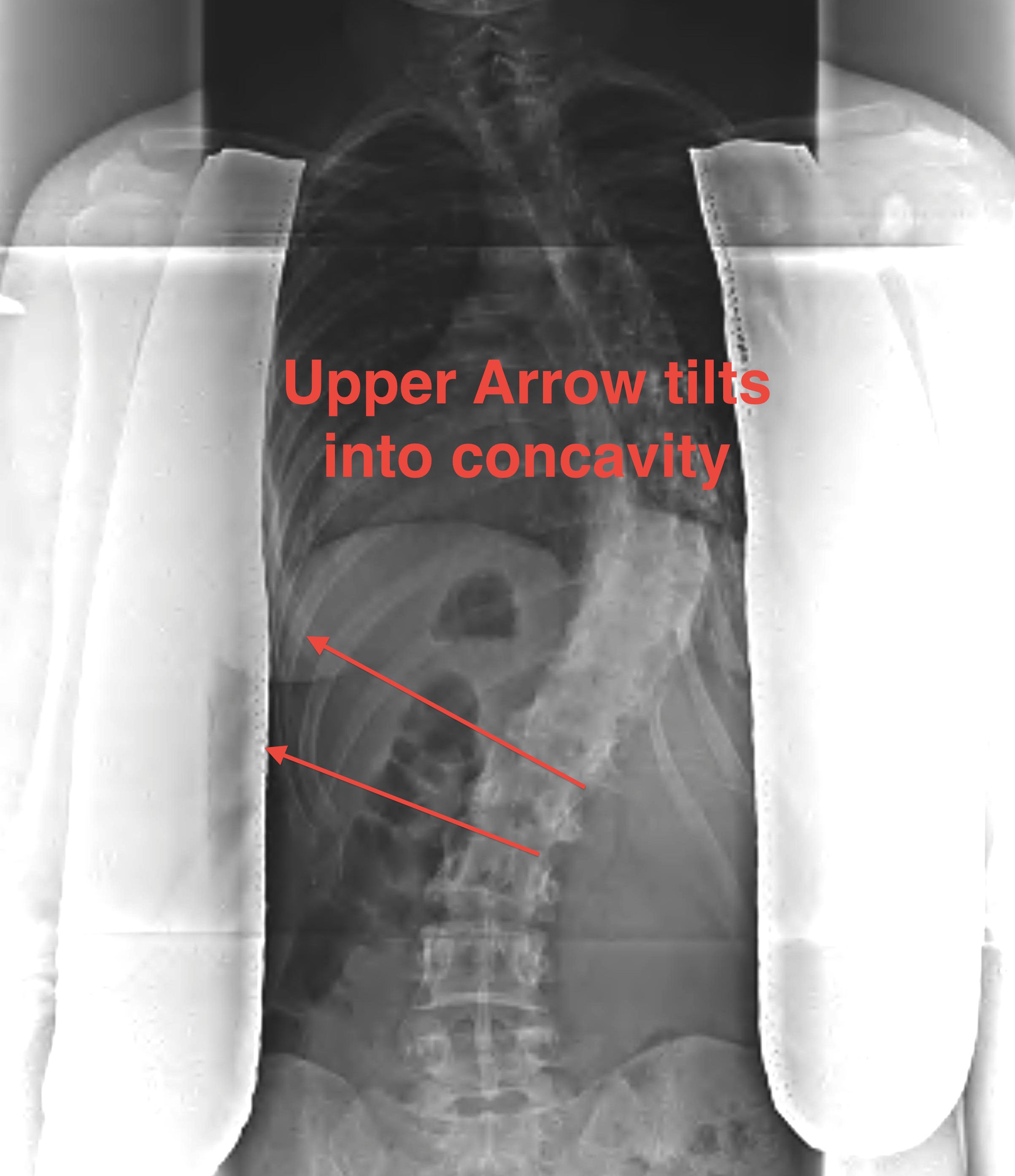
1. Neutral / end vertebrae
End vertebra is the last vertebra that tilts into the concavity of the curve
- when the end plates are parallel, the one furthest from the apex of the curve is the end vertebra
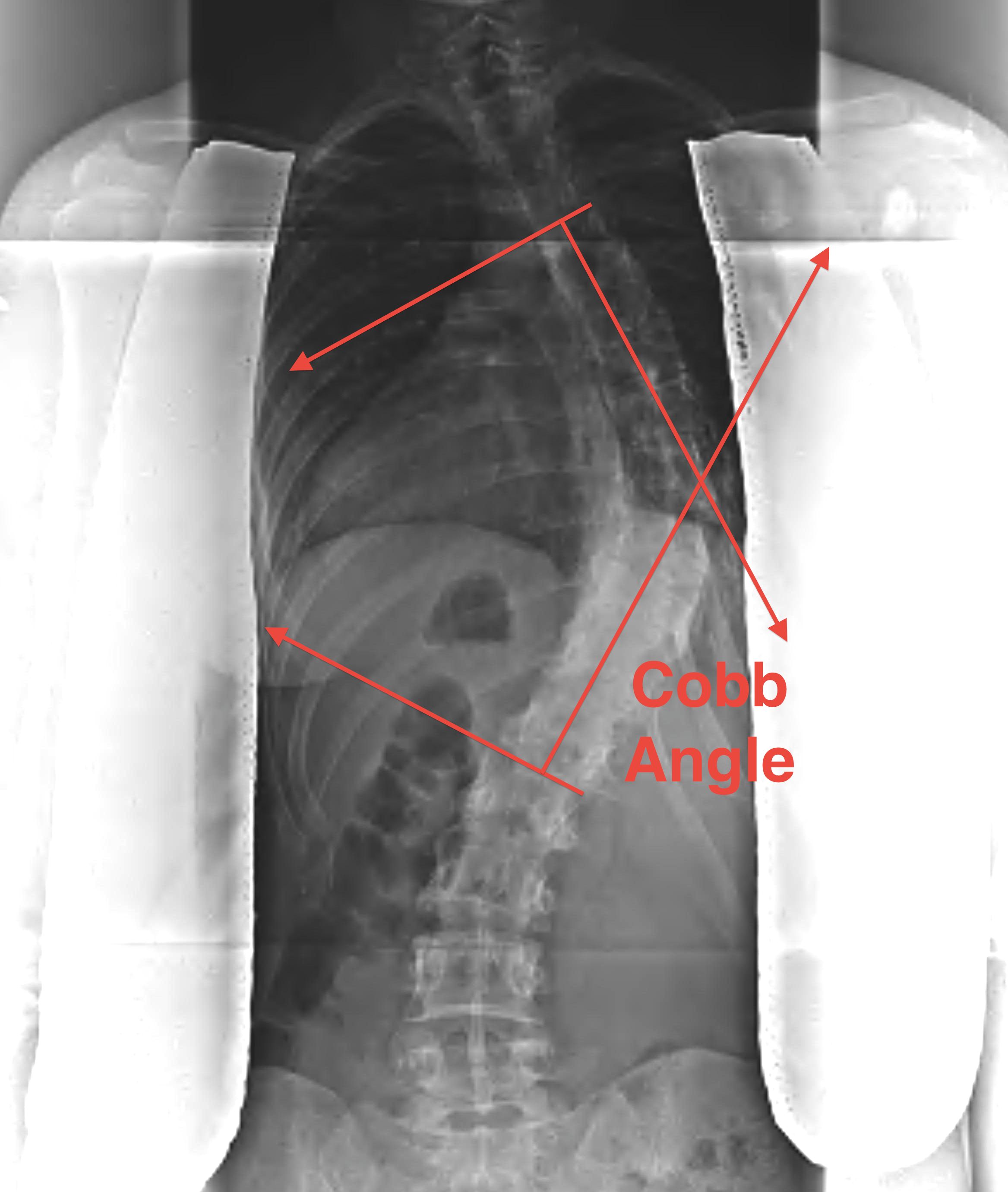
2. Cobb Angle
Detect the end vertebrae where the end plates are last to converge
- line drawn along upper plate of the upper end vertebrae and lower plate of the lower end vertebrae
- perpendiculars to these lines
- intersection angle measured
If double curve
- one vertebrae is upper end vertebrae for the lower curve
- lower end vertebrae foe the upper curve
Measurements all taken from same vertebrae in future
3. Identify Apical Vertebrae
In centre of curve
- furtherest from central sacral line
- not tilted / most horizontal
- maximum rotation
T10 above apical - Thoracic
T11 - L1 apical - Thoracolumbar
L2 down - Lumbar
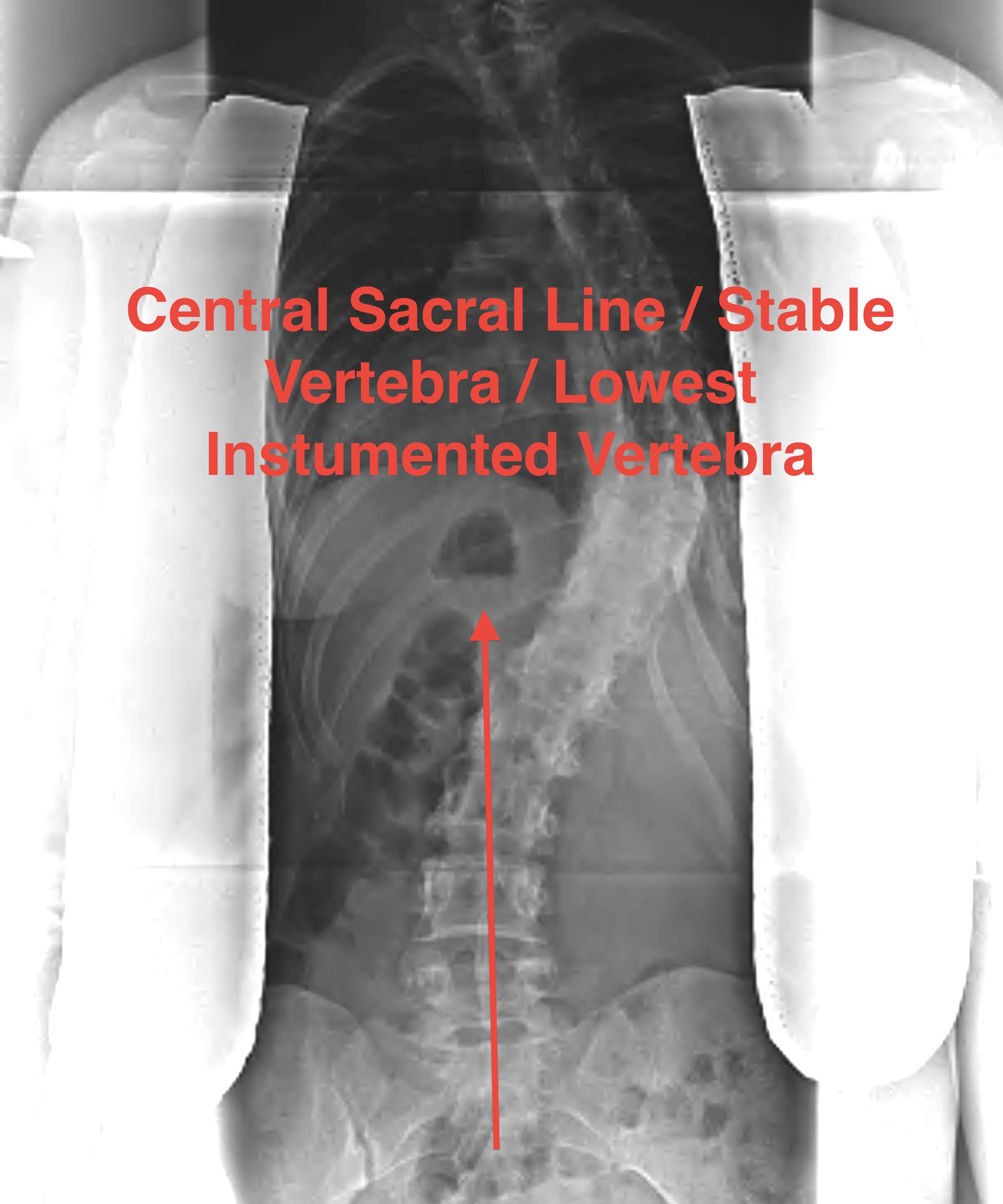
4. Stable Vertebrae
Central sacral line
- lowest vertebrae this bisects or
- line between 2 pedicles
- lowest vertebrae instrumented in surgery
5. Look at shoulders
Important in double thoracic major
- high structural thoracic curve
- if left shoulder high in right thoracic curve
- need to instrument to T2 to correct this
Lateral Films
Standing
- measure the kyphosis and lordosis via Cobb method
- important presurgery
- want to correct this intra-operatively
- usually need to recreate thoracic kyphosis
Lateral Bend Films
Push prone
- supine with maximal voluntary bend
- differentiates structural from compensatory curves
MRI
If suspect intraspinal pathology
- Brain + 3 level spine / neurocentral
Indications for MRI

Left sided
Male
Painful
Rapidly progressive
Neurological abnormality present
Findings
Right sided curve: 20% have pathology
Left sided curve: 80% have pathology
Assessment of Rotation
Rib Hump / Scoliometer
Adams forward bend test
< 5o tilt = < 30o rotation
> 7o tilt = > 30o rotation
Rotation of Pedicles
- indicates the structural curve
Classification
Lenke
3 areas of curve
- main thoracic: MT
- proximal thoracic: PT
- thoracolumbar / lumbar: TL/L
Assess
- curve location
- lumbar modifier
- thoracic sagittal profile
Type 1 Main Thoracic
- MT structural
- PT non structural
- TL/L non structural
Type 2 Double Thoracic
- MT and PT structural
- TL/L non structural
Type 3 Double Major
- MT and TL/L structural
- PT non structural
Type 4 Triple Major
- all 3 structural
Type 5 Thoracolumbar / Lumbar
- only TL/L
Type 6
- TL/L and MT structural
- TL > MT by more than 10o
King-Moe Classification
Very poor inter observer reproducibility
Type I - Lumbar Dominant Double T + L
- both the thoracic and lumbar curves cross the midline
- lumbar curve larger and more rigid
Type II - Thoracic Dominant Double
- both the thoracic and lumbar curves cross the midline
- thoracic curve larger and more rigid
Type III - Short Thoracic
- thoracic curve
- lumbar curve doesn't cross the midline
- lumbar curve not structural
Type IV - Long thoracic
- long thoracic curve extends to lumbar spine
- L5 over the sacrum
- L4 tilted into the curve (stable vertebrae)
Type V - Double structural thoracic
- double thoracic curve with L upper, R lower
- tilting of T1 into the upper curve / elevation of L first rib
- cervical extension
- compensatory lumbar curve with upper curve structural