Options for MCL
Repair
Reconstruction
Femoral repair of MCL
Tibial repair of MCL
MCL Reconstruction options
1. Single graft PCL / MCL reconstruction
Single femoral tunnel
- intra-articular - PCL femoral insertion
- extra-articular: exits at medial femoral condyle
Wahl and Nicandri Arthroscopy 2008
2. MCL tendoachilles reconstruction (single bundle anatomic)
Medial approach to femur
- divide retinaculum
- elevate VMO
Femoral tunnel
- identify adductor tubercle with insertion of adductor magnus
- insertion of superficial MCL is 12 mm distal and 8 mm anterior to adductor tubercle
- insertion of superficial MCL is just proximal and posterior to the medial epicondyle
- xray: the intersection of the posterior femoral cortex and blumenstaat's line
Tibial attachment
- 6 cm below joint line
- posteromedial tibia
- posterior to pes anserinus attachment
Marx technique MCL reconstruction with tendoachilles allograft PDF
Marx technique MCL reconstruction with tendoachilles allograft Vumedi
3. Hamstring allograft reconstruction (single or double bundle anatomic)
Issues
Avoiding femoral tunnel convergence of MCL with PCL
- aim femoral MCL tunnel 40o anterior and 40o proximal
Technique ACL (hamstring autograft), PCL (tendoachilles allograft) and MCL (tendoachilles allograft) reconstruction
Laprade ACL / PCL / MCL surgical technique PDF
ACL / PCL
Graft Preparation


1. Achilles allograft for PCL
- generally split graft into two
- 9 mm wide x 20 mm long bone block (for 10 x 25 femoral drill hole)
- 2 x drill holes with 2 x high strength suture
- tubularise distal end of tendon and leave long sutures
- ensure passes easily through 9 mm tunnel
2. Achilles Allograft for MCL
- split the achilles allograft
- 8 mm wide x 20 mm long bone block (for 9 x 25 femoral drill hole)
- 2 x drill holes with 2 x high strength suture
- don't tubularise or whipstitch the tendon end
3. Harvest and prepare hamstring tendons
- medial incision
- ACL and PCL tibial tunnels will pass through this incision
- will also secure tibial sided MCL reconstruction in this incision (most posteriorly)
- place over endobutteon
- size as normal
Arthroscopy
Debridement of notch
Place posteromedial cannula
- most common mistake is placing cannula too anterior / inferior
- need to be able to instrument PCL origin
- also allows direct visualisation with camera
Assess / treat meniscus
PCL Tibial Tunnel

Change to 70o scope
- under vision clear PCL facet
- release posterior capsule from bone (visualise popliteus muscle)
- release posterior speptum (attaches to PCL, and divides knee into posteromedial and posterolateral)
- PCL guide 65o angle
- tibial guide placed just lateral to crest to ensure room for more medial ACL tunnel
- place on posterior facet, slightly lateral
- check on fluoroscopy on PCL facet
- protect guide wire with curette or switching stick via PM cannula
- carefully ream 10 mm tunnel
- clear tunnel entrance of debris
PCL femoral tunnel


Open incison medial knee
- elevate VMO
- use PCL jig and place in centre of anterolateral bundle
- ensure sufficient distance from anterior articular cartilage
- also ensure sufficient distal from the MCL tunnel (just posterior and proximal to medial epicondyle)
- drill 10 mm tunnel for achilles bone block from outside-in or inside-out
ACL
Drill appropriate size tibial and femoral tunnel
- hamstring tendon technique
- set jig to 550 to miss PCL tunnel
- ensure is in more medial aspect of the tibial tunnel
PCL graft passage
Option 1
- pass from outside in
- suture up tibial tunnel, and up femoral tunnel
- pass graft tendon first from femoral tunnel
- secure outside in with 7 or 8 mm metal screw
Option 2
- pass PCL graft through small lateral parapatella approach (enlarge portal)
- looped suture up tibial tunnel and out anterolateral portal
- looped suture down femoral tunnel and out anterolateral portal
- pass graft into knee
- tendon passes down tibial tunnel
- manipulate bone plug into femoral tunnel
- secure femoral side inside out with 7 or 8 mm metal screw

ACL graft passage
As per normal technique
- flip endobutton
- don't secure tibial end

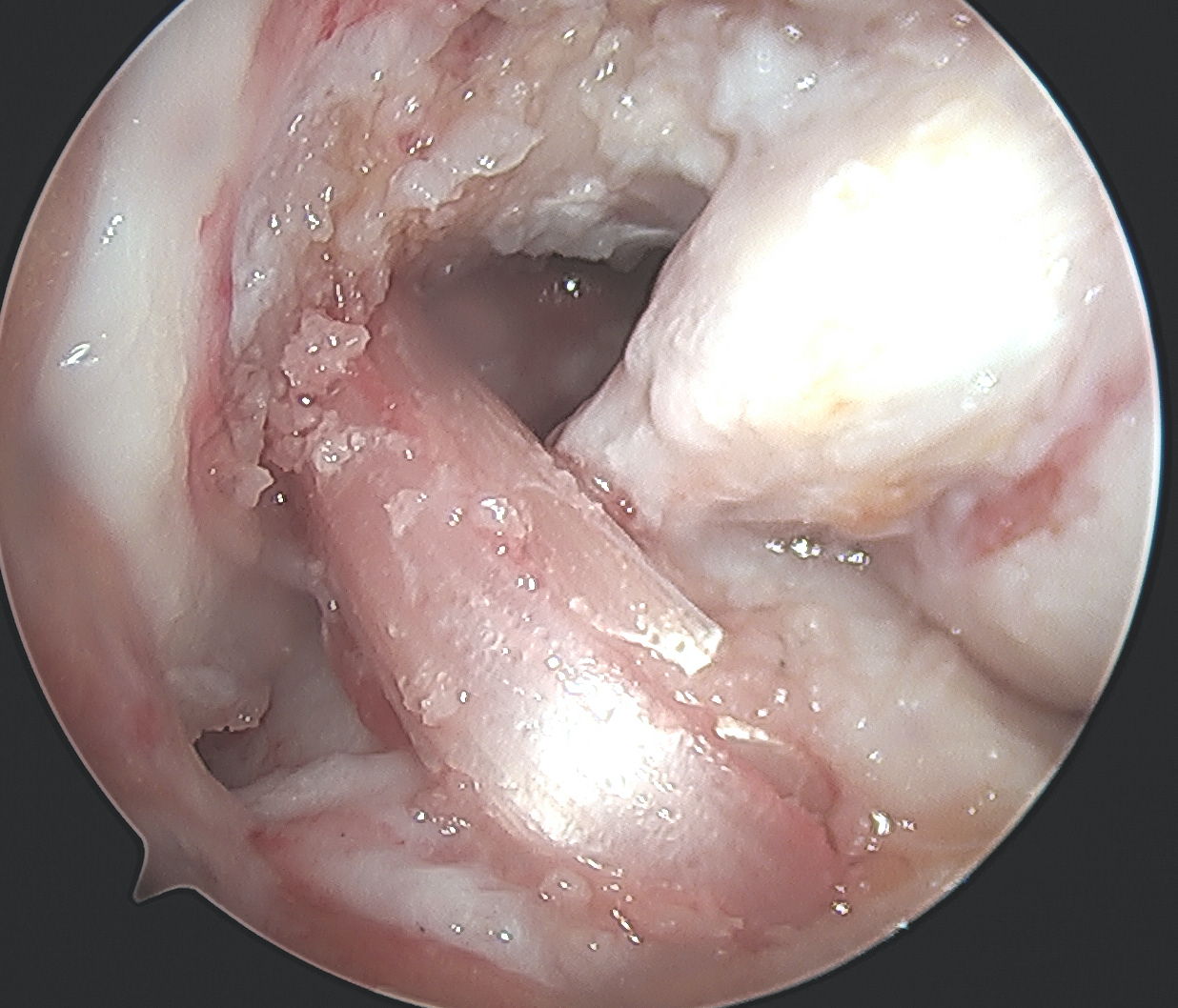
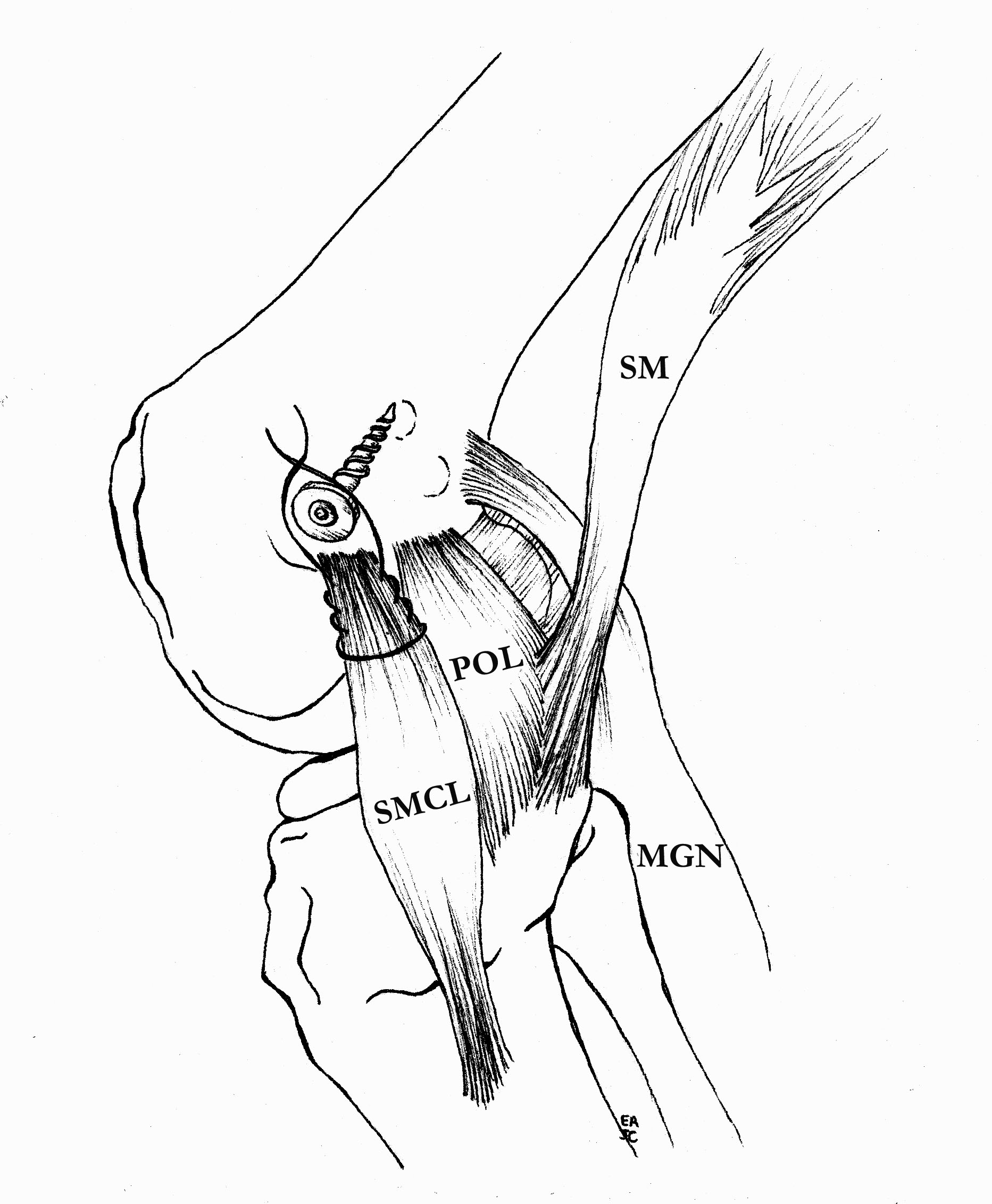
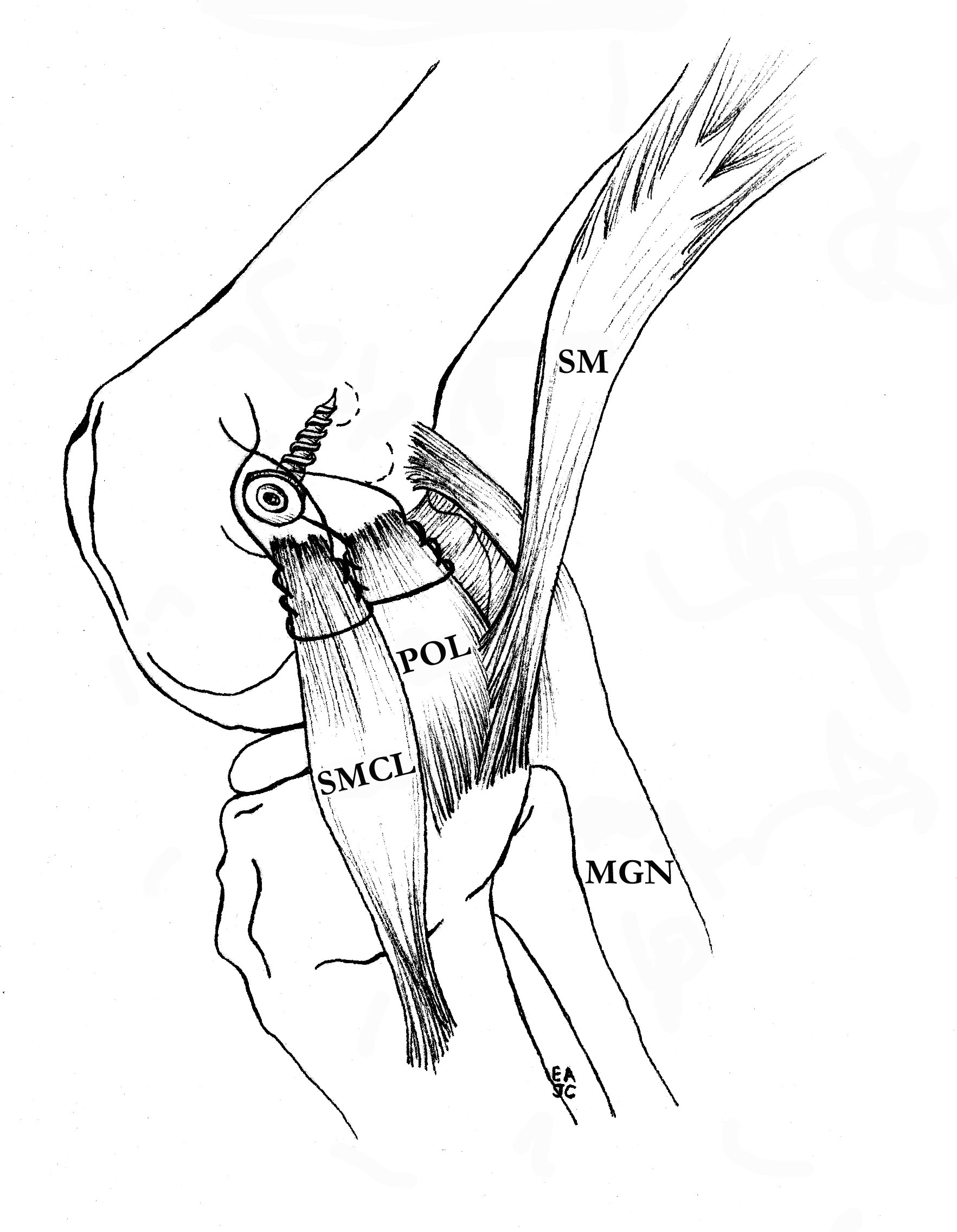
MCL Reconstruction
Femoral side
- use previous proximal medial incision
- identify PCL femoral tunnel
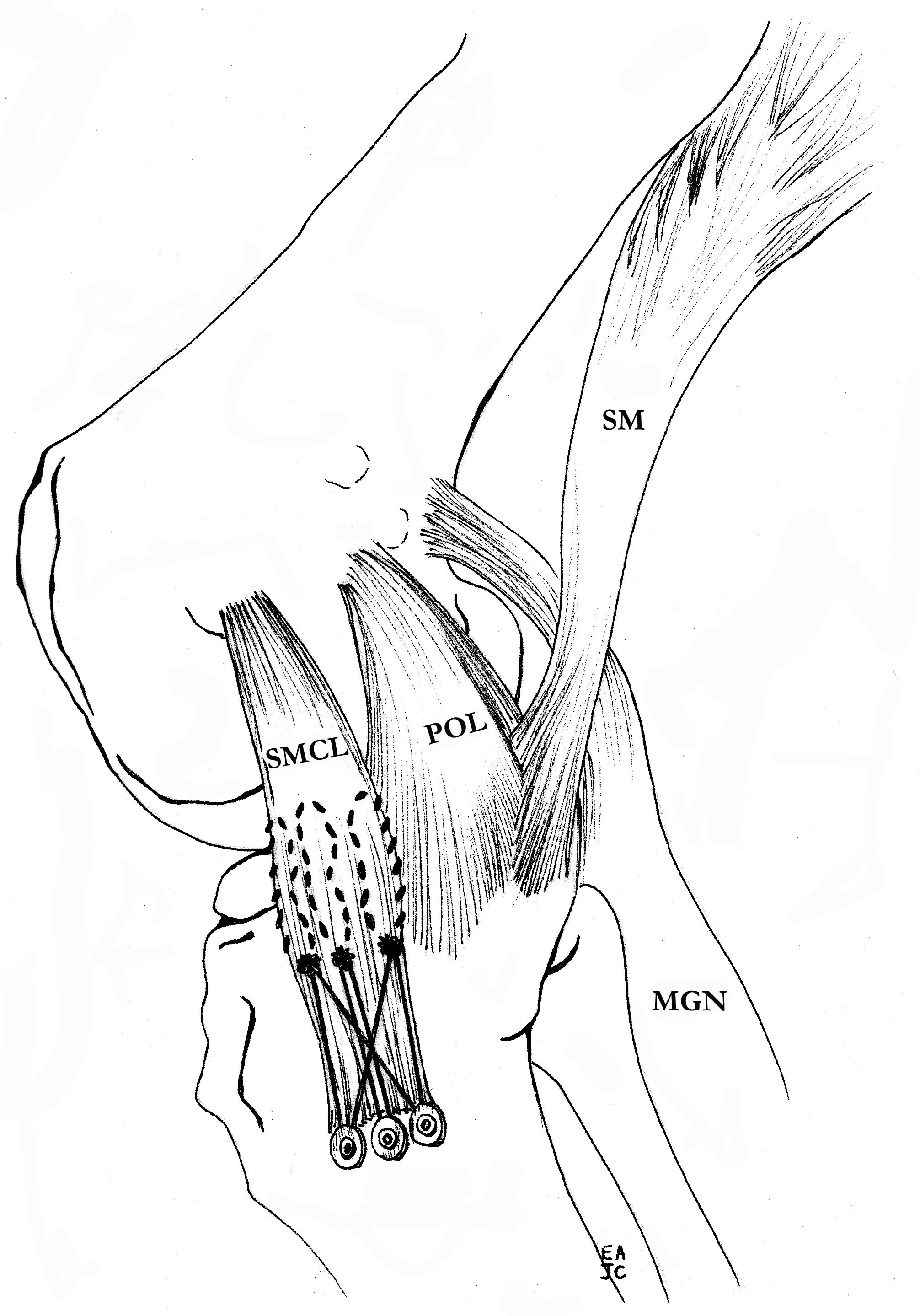
MCL insertion
- identify adductor tubercle (insertion point of adductor magnus tendon)
- medial epicondyle is 12 mm distal and 8 mm anterior to adductor magnus
- insertion point of MCL is 4 mm proximal and 4 mm posterior to medial epicondyle
- can use xray (intersection of the posterior femoral cortex and blumenstaat's line)
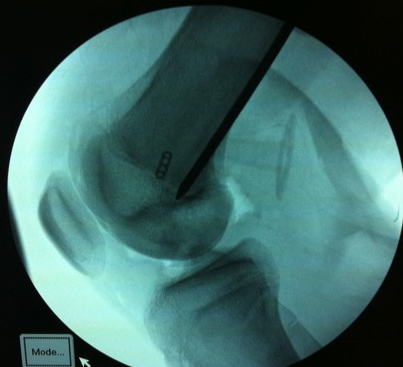
Drill MCL femoral tunnel
- 9 x 25 mm
- aim 40o anterior and 40o proximal to avoid PCL tunnel convergence
- insert bony plug and fix with a 7 x 20 mm metal screw
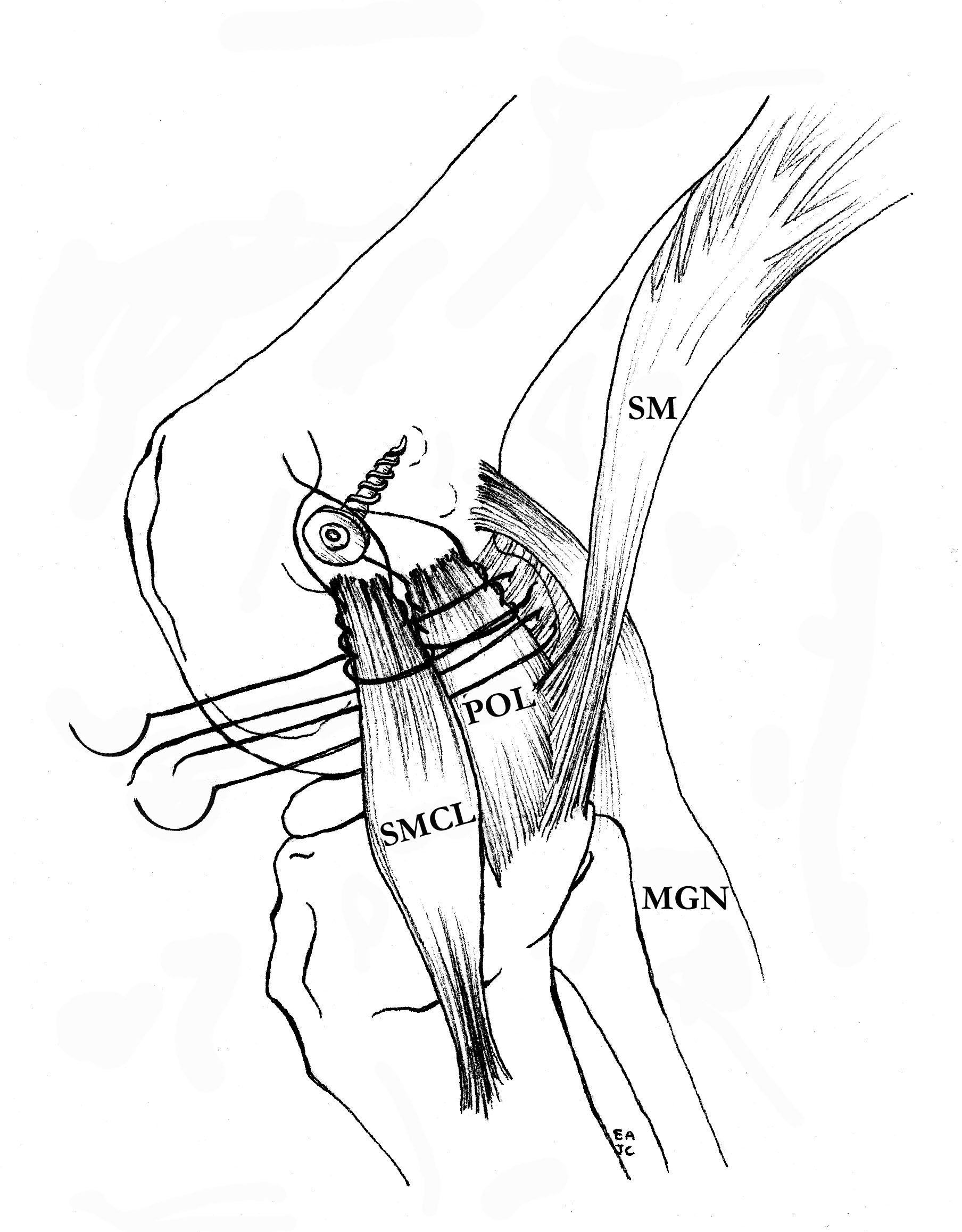
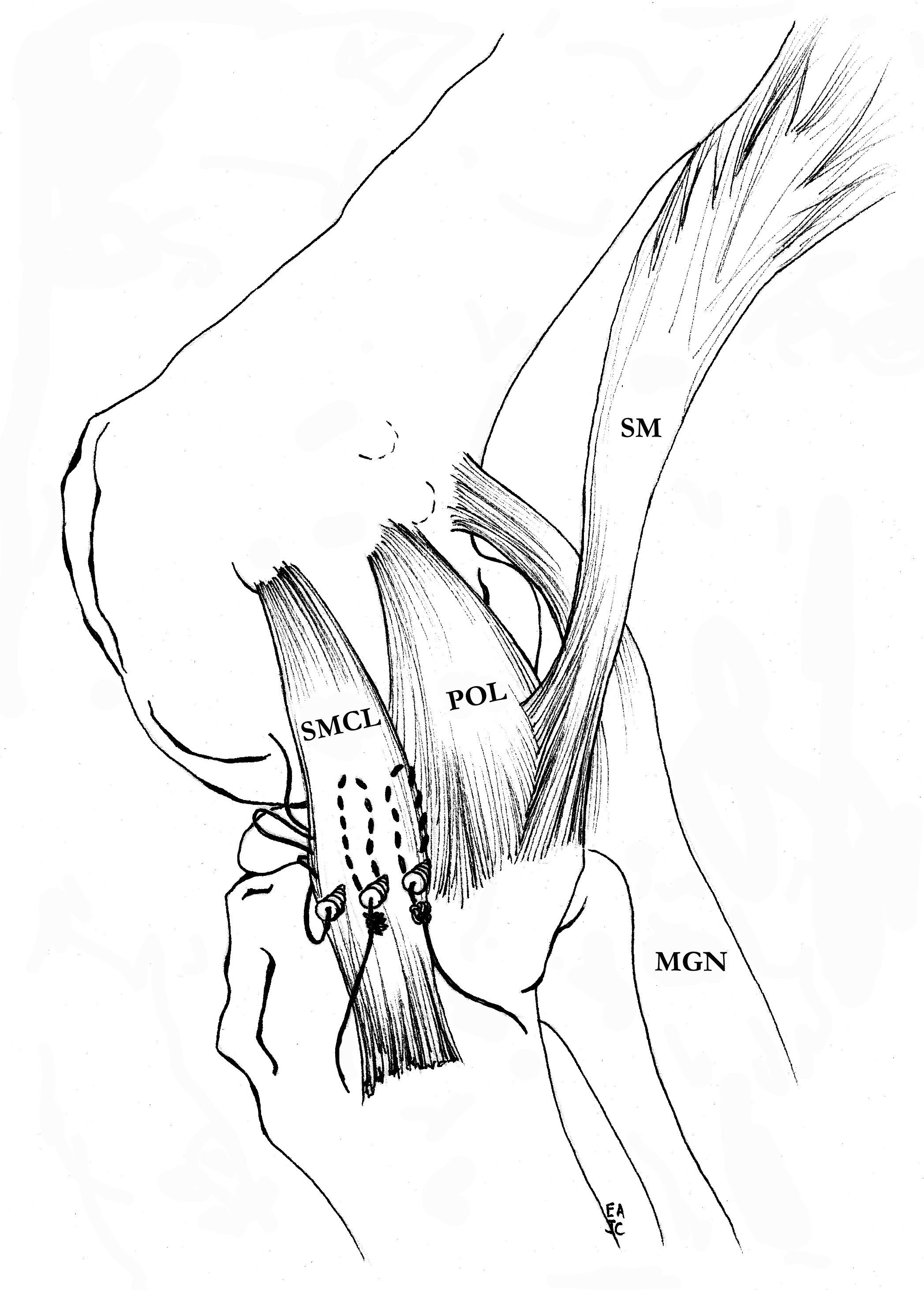
MCL tibial fixation
- use instruments to make passage for tendon end of achilles allograft
- fixation point is 6 - 7 mm below tibial joint line
- use a 4.5 mm cortical screw from large fragment set
- use a spiked soft tissue washer from the large fragment set
- can place soft tissue anchors on proximal tibia for two point fixation
Tibial sided graft fixation
1. PCL - 90o
2. ACL - 30o
3. MCL - 30o with varus force and foot in neutral
PCL
- 90o
- pull tibia forward
- tension graft +++
- because the tunnel on the tiba is very anterior, bone is very hard
- line to line screw, may need to downsize
- 8 x 35 screw (longer as tunnel is longer)
- have anterior draw on tibia and foot IR
- secure with post / staple

Post operative rehabilitation
NWB for 6 weeks
ROM to 90o
Hinge brace for 6 weeks
Consider PCL brace
After 6 weeks full ROM and FWB
Consider hinge brace for 3 months
No sport for 1 year due to allografts