Definition
Anterior displacement of peroneal tendons out of peroneal groove
Epidemiology
Most common in young adults
Acute injury often missed
Aetiology
Congenital
3 % neonates
- resolves spontaneously
Traumatic
Occurs following sporting activities
- snow skiing
- football
- gymnastics
Forced DF and inversion
Anatomy
Fibro-osseous tunnel
- retro-malleolar groove
- lined by fibrocartilage
Anterior
- fibula
Medial
- PTFL
- CFL
- PITFL
Peroneus longus
- posterolateral to PB
Superior Peroneal Retinaculum
- 2 bands
- fibula to lateral T Achilles
- fibula to posterolateral calcaneum
Inferior peroneal retinaculum
- lateral wall calcaneum below sinus tarsi
- no role in stability
Pathogenesis
1. Traumatic
Violent contraction of Peroneal muscles
Forced dorsiflexion and inversion
- injury to superior peroneal retinaculum
May be predisposition
- laxity of retinaculum
- shallow groove
Patient may also have tears
2. Subluxation within sheath
Raikin JBJS Am 2009
- described intrasheath subluxation
- superior retinaculum intact
- patients still having painful snapping
- demonstrated by US
- half had peroneal tendons switching positions
- these patients had a convex groove
- these where treated with groove deepening and retinaculum reefing
- other half had a tear in PB through which PL could sublux
History
Acute
- sudden pain behind lateral malleolus
- snap may be heard
- unable to continue with activities
Chronic
- painful snapping of lateral ankle with activity
Examination
Tenderness & swelling behind LM
- pain or dislocation reproduced by active eversion & DF


X-ray
Usually normal
May be avulsed fragment of cortical bone lateral to LM
- fleck sign
CT
Defines anatomy & relationships of tendons
- may detect anatomical variants
US
Very good at demonstrating subluxation
MRI
Detects tendinous & ligamentous injuries
Management
Opinion divided regarding acute injuries
- non-operative management v surgical repair
Most treat chronic injuries surgically
Non-operative
Acute injuries
- cast in plantarflexion for 6/52
Operative
Indications
- acute injury in athletes
- chronic injuries
Acute Repair
Options
1. Superior retinaculum stripped
- reattach to fibula via trans-osseous sutures / anchors
2. Retinaculum torn
- primary repair
3. Bony avulsion
- fragment reattached with sutures, wires or screws
Chronic
1. Groove Deepening
- if necessary
- elevate cortical flap / decancellation / cortical recession
2. Address tears in tendons
3. Address superior peroneal retinaculum
A. Direct repair / Advancement of superior peroneal retinaculum if able
B. Reconstruction of SPR if attenuated
- periosteal flap from fibula
- slip of T Achilles left attached distally
- free plantaris / palmaris graft
C. Rerouting under CFL
- substitution of CFL for peroneal retinaculum
- tendons transposed into inframalleolar tunnel
- division & repair CFL or fibular bone block with CFL
4. +/- lateral ligament repair if needed
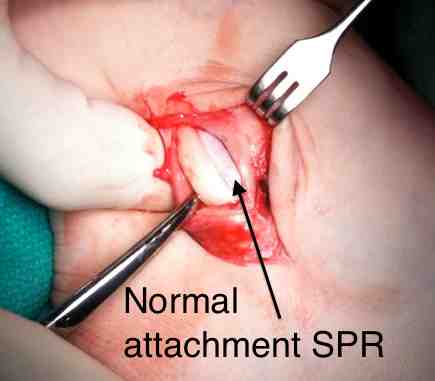
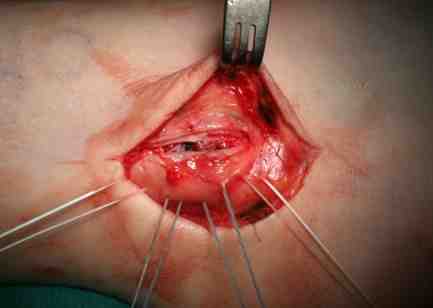
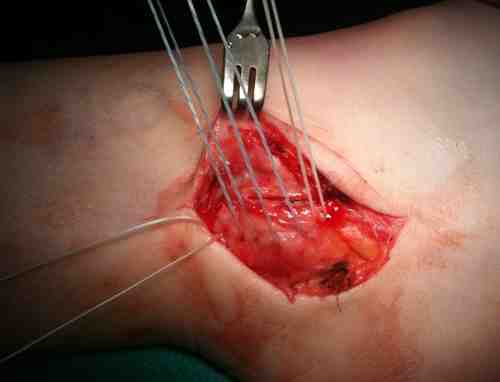
Surgical Technique
Findings
- chronic subluxation / anterior dislocation
- normal groove
- retinaculum stretched and not attached to normal insertion anterior fibula
- repair and tightened with suture anchors