Definition
Pain at attachment of thickened central part of plantar aponeurosis to Medial Calcaneal Tuberosity
Anatomy Plantar Fascia
Origin
- medial calcaneal tuberosity
Inserts
- 5 bands superfical & deep layers
Superficial
- insert transverse MT ligament & skin
Deep
- flexor sheath, volar plate & periosteum of P1
Action
- when toes passively DF in toe off
- inelastic
- stabilises and elevates arch of foot
- windlass mechanism
Fat Pad
- absorbs 20-25% of force at heel strike
- U-shaped, fat arranged in fibro-elastic septa
Epidemiology
Usually middle-aged male
- age 40-70 years
- M:F = 2:1
- usually unilateral
Predisposing factors
- obesity
- certain occupations i.e. Policeman's heel
- athletes and repetitive stress
Aetiology
Usually idiopathic
May be associated condition especially if bilateral
- Reiter's Disease
- Ankylosing Spondylitis (enesopathy)
- Gout
Pronated feet / cavus feet / planus feet
Obesity
Tight tendoachilles
Theories
1. Degenerative change fat pad most common finding
- decreased ability to cushion heel
2. Injury to windlass mechanism with micro trauma
3. Nerve entrapment
4. Heel spur present in 50% with heel pain
- spur is in origin FDB (short flexors) not plantar fascia
Shmokler 1000 patients
- 13.2% incidence heel spurs
- 5.2% of which had heel pain
Williams
- 45 patients 52 painful heels
- 75% painful heels with spur
- 65% opposite heel had spur

Pathogenesis
Degeneration 80%
Repetitive stress at attachment
- leads to microscopic tears & cystic degeneration
- maybe periosteal reaction & spur formation
Entrapment 20%
Nerve Entrapment Syndrome
- lateral plantar nerve / Baxter's nerve
- mixed motor and sensory
- motor to abductor digiti minimi
- runs superior to plantar fascia
- may be compressed by spur or fascia
- difficult to diagnose
History
Pain at inferomedial aspect of heel
- worse when first rising from bed
- worse with prolonged standing or extreme exercise
Examination
Local tenderness at inferomedial aspect of Calcaneal tuberosity
Pain aggravated by passive dorsiflexion of toes
Tinel's sign
Cavus / Planus
Tight T Achilles
X-ray
Maybe calcaneal spur (50%)
- exclude tumour & infection
Bone Scan
Can be useful in atypical presentations
MRI
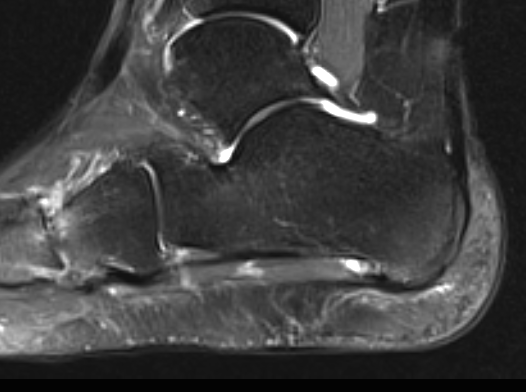
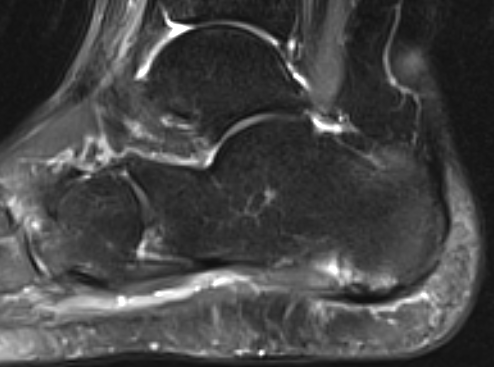
Inflammation of the plantar fascia at its insertion
May show compression of 1st branch of lateral plantar nerve
DDx
Inferior heel
- calcaneal stress fracture
- fat pad atrophy
- calcaneal apophysitis
- nerve compression / tarsal tunnel
Posterior heel
- Achilles tendonitis
- retrocalcaneal bursitis
- STJ OA
NHx
80-95% settle with non-operative management
- in 6-12/12
Management
Non-operative
Acute cases respond better to HCLA
Chronic better to orthoses
Soft Heel Cup with Instep
Physiotherapy
- T Achilles stretches
- Plantar fascia stretches
- can rolling
Orthoses
- well padded running shoes
- viscous heel cushions + longitudinal arch support
- Soft Heel Cup with Instep
Night splint
- hold in 15o DF
- very effective
- maintain night-time stretch
NSAIDS
ECSW
Aqil et al. CORR 2013
- meta-analysis of RCTs
- safe and effective treatment
- effects evidence at 12 weeks, last up to 12 months
High energy ECSW v low energy ECSW
- evidence for both
Cast immobilisation
- keeps plantar fascia under constant stretch and minimises microtrauma
- patient should undergo this treatment before consideration for surgery
- very effective treatment
Injections
Cortisone
- ? US guided
- max 2 (plantar fascia can rupture)
PRP
Acosta-Olivo et al. J Am Podiatr Assoc 2016
- RCT of cortisone v PRP
- equally efficacious
- no between group difference
Botox
Ahmed et al Foot Ankle Int 2016
- RCT of saline v Botox
- significant improvement in botox group
Operative
Indication
- must have minimum 12 months non-operative treatment
- 5% of patients
- results of surgery variable
Results
Contompasis
- 129 patients
- 43% complete improvement
- 38% some improvement
- none worse off
Open Release of Plantar Fascia
Set up
- tourniquet
- prone / lateral / supine
Incision
- medial longitudinal incision
- this is often vertical in line with posterior border medial malleolus
- protect medial calcaneal branch
Dissection
- divide ABHB fascia
- reflect this superiorly
- identify plantar fascia origin from tuberosity
- FDB is above plantar fascia
- insert homan retractors above and below
- lateral plantar nerve deep to abductor, above FDB laterally
Resection
Resect medial rectangle of plantar fascia
- divide 3/4 of fascia
- don't release in full unless very old and decrepit
- take 6 deep by 2 mm thick rectangle
+/- neurolysis
+/- Resect spur
- reflect FDB
- remove with osteotome / nibbler
B. Endoscopic release
Ogilvie-Harris Arthroscopy 2000
- 53 patients with 65 feet
- complete resolution of pain in 89%
- 71% returned to unrestricted sport
Results
Cochrane Review 2012
- no evidence for laser or ultrasound
- limited evidence for dorsiflexion night splints
- limited evidence topical corticosteroid
- some evidence for injected CS
- equivocal for ECSW