Advantages
Improved cosmesis
Shorter hospital stay / less immediate post operative pain
Deltoid not detached
Ability to evaluate and treat coexisting intra-articular pathology i.e. biceps
Disadvantage
No quicker to rehab or return to activities
- limiting factor is healing of tendon to bone
- healing rates not as high especially for large to massive tears
- steep learning curve / longer surgery
Issues
1. Footprint
- 25 x 15 mm
- healing zone
- the greater the extent a repair covers, the greater the chance for tendon bone healing
2. Suture technique
Note: Most common means of failure is suture cutout
A. Open transosseous
Technique
- performed in open surgery
- captures a wide section of cuff footpring
- very secure repair with uniform compression between cuff and bone
B. Single row repair
Technique
- anchors placed in line laterally at insertion
C. Double row repair
Technique
- medial anchor row at articular margin
- lateral anchor row at lateral footprint
Kim et al Am J Sports Med 2006
- biomechanical study
- more successful at restoring footprint
- less gap formation
- increased load to failure
D. Transosseous equivalent / suture bridge
Technique
- biomechanically replicate tradional open transosseous
- sutures crossed as below in double row
- aiming to increase contact between cuff and footprint
Siskoksy et al AAOS 2007
- biomechanical study suture bridge v double row
- bridge higher load to failure
- no difference in gap formation
Results
Outcome arthroscopic
Lafosse et al AA Should Elbow Surgeons 2006
- 105 patients treated with double row
- 11.45 structural failure on CT / MRI
Sugaya et al JBJS Am 2007
- prospective study 106 FT
- arthroscopic double row
- MRI follow up
- 17% retear
- 5 % small to medium
- 40% large and massive
Arthrocopy v mini-open
Kim et al Arthroscopy 2003
- arthroscopy v mini open
- similar outcomes in each group
- poor outcome related to size of tear, not method of repair
Verma et al Arthroscopy 2006
- arthroscopy v mini open
- US review
- 24% retear mini-open
- 25% retear arthroscopic
- no difference in outcome
Bishop et al AAOS 2004
- mini open v arthroscopic
- MRI review
- tears < 3 cm: 26% retear mini open, 16% arthroscopic
- tears > 3m: 38% v 76%
- do larger tears do better with open surgery?
Morse et al Am J Sports Med 2008
- meta-analysis of arthroscopic v open
- no difference in outcome or complications
Single v Double Row
Francheschi et al Am J Sports Med 2007
- RCT single v double row
- 60 patient
- no difference functional outcome
- improved cuff appearance on MRI
Burks et al Am J Sports Med 2009
- RCT single row v double row
- 20 in each group
- 1 retear in each group
- no difference in MRI appearance or clinical outcome
Cost
Churchill et al J Should Elbow Surg
- arthroscopic took average 10 minutes longer / cost $1000 dollars more
- even at high volume centres
Arthroscopic Supraspinatous Repair
Technique
Position
- lateral decubitus with arm traction 10 lb or
- beachchair in Tmax / Spyder (can depress arm and ER to aid visualisation)
- water pump
- useful to have adrenalin in bags
- stable BP 110 (interscalene block can help)
- inject LA with A into subacromial space and prospective portals
Portals
Posterior Portal
- make more superior and lateral
- awkward for GHJ arthroscopy
- good visualisation in subacromial space
- will put camera over and high above tear
Lateral portal
- standard position
- insert large 8 mm cannula (will need to pass sutures)
- perform bursectomy +++ for visulisation
- bursa posteriorly and medially often bleeds
- perform SAD
- control bleeding with electrocautery and temporary increases in pump pressure
Anterior portal
- smaller 6 mm
- for suture shuttling
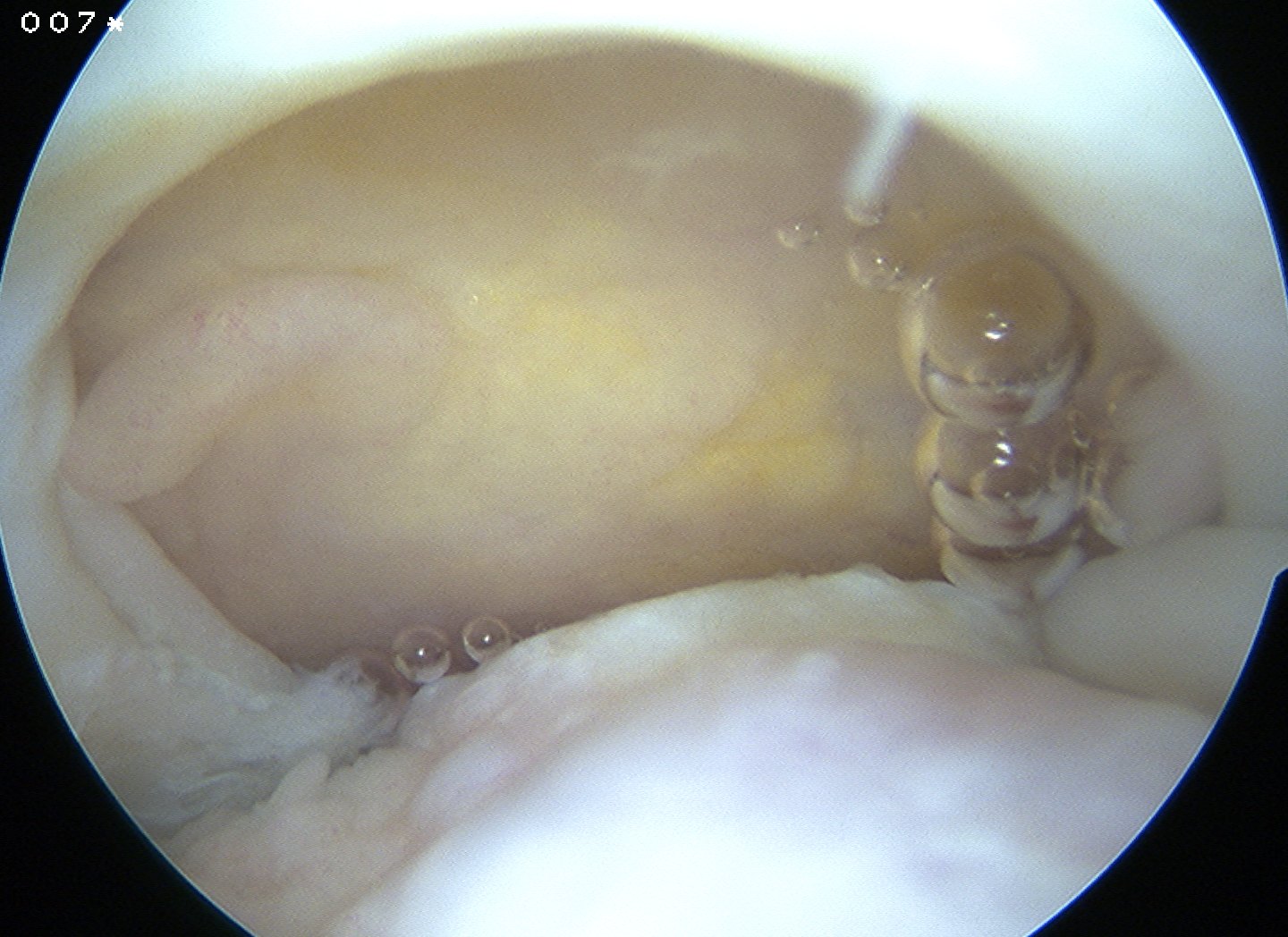
Preparation
Prepare insertion
- debride tendon edges
- debride footprint to punctate bleeding
Assess tendon mobilisation / tear geometry
- perform releases if needed
- as per open surgery
- above and below tendon 1 cm medial to glenoid
- release coracohumeral ligament
Repair
Large U shaped tendon
- insert margin convergence sutures
- put camera in lateral portal
- insert posterior cannula over switching stick
- anterior and posterior bird beaks
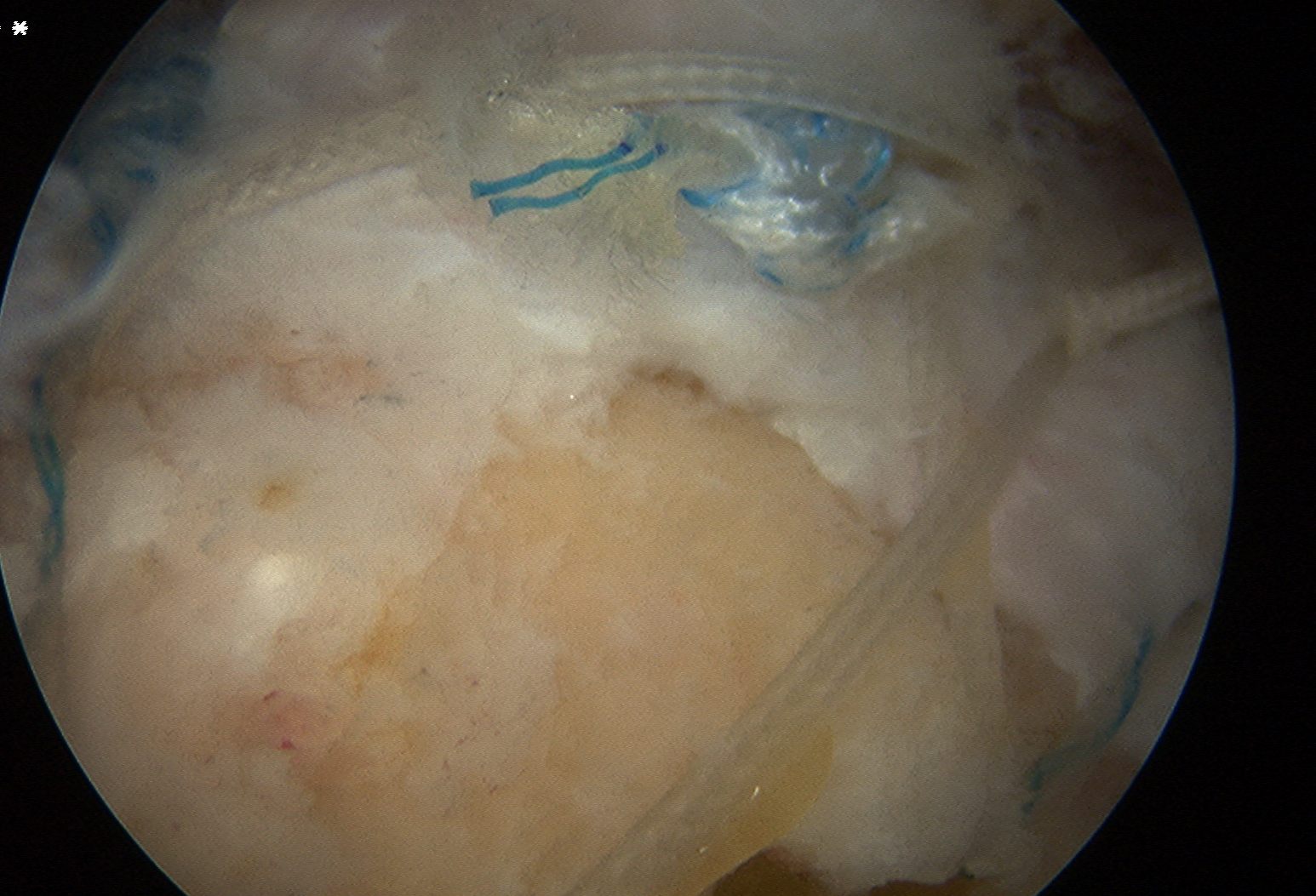
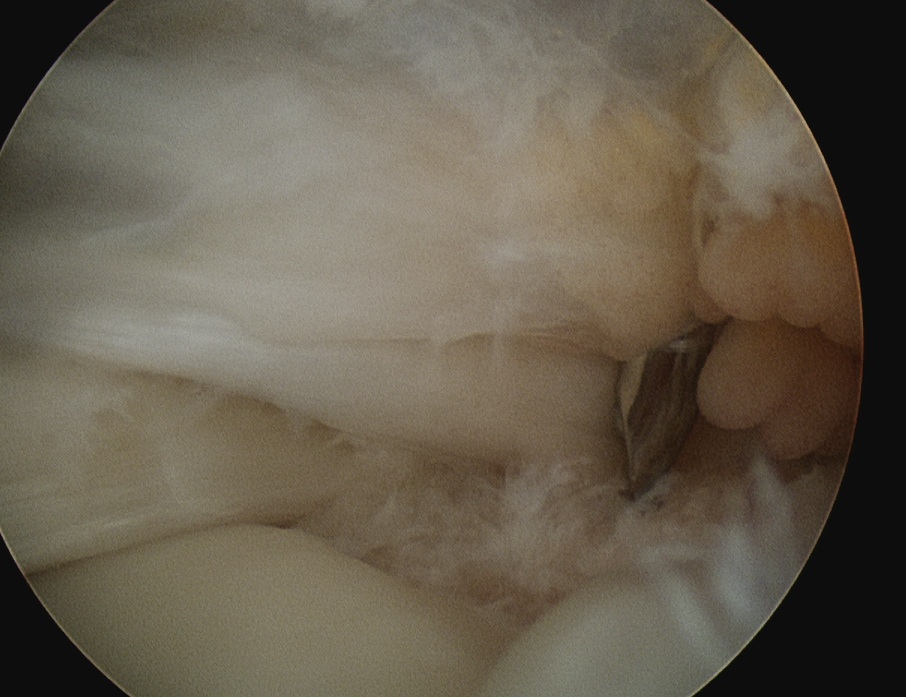
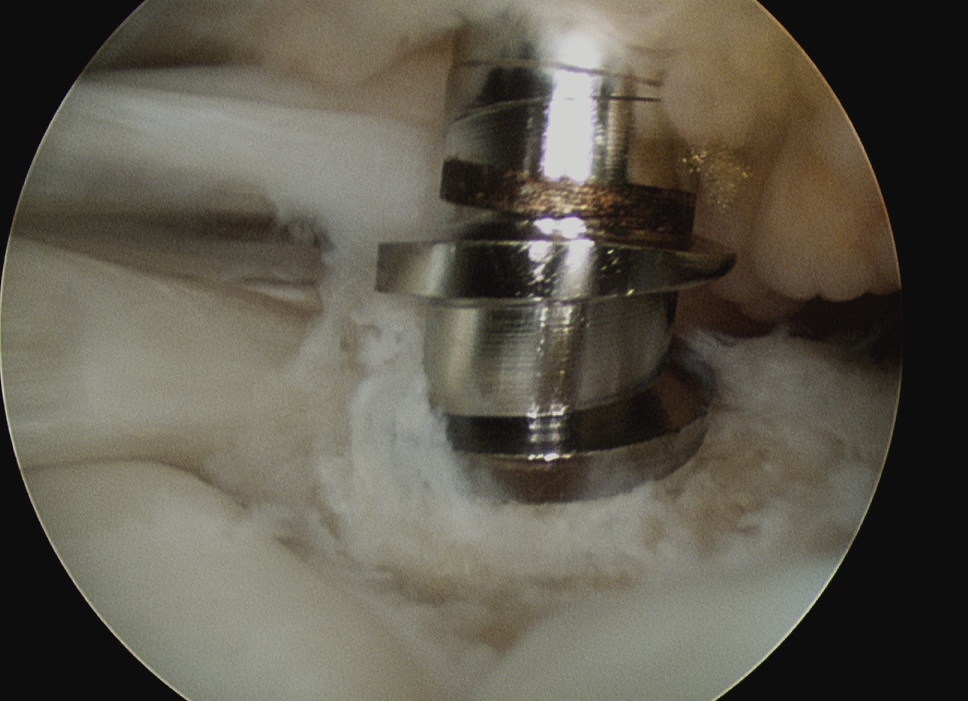
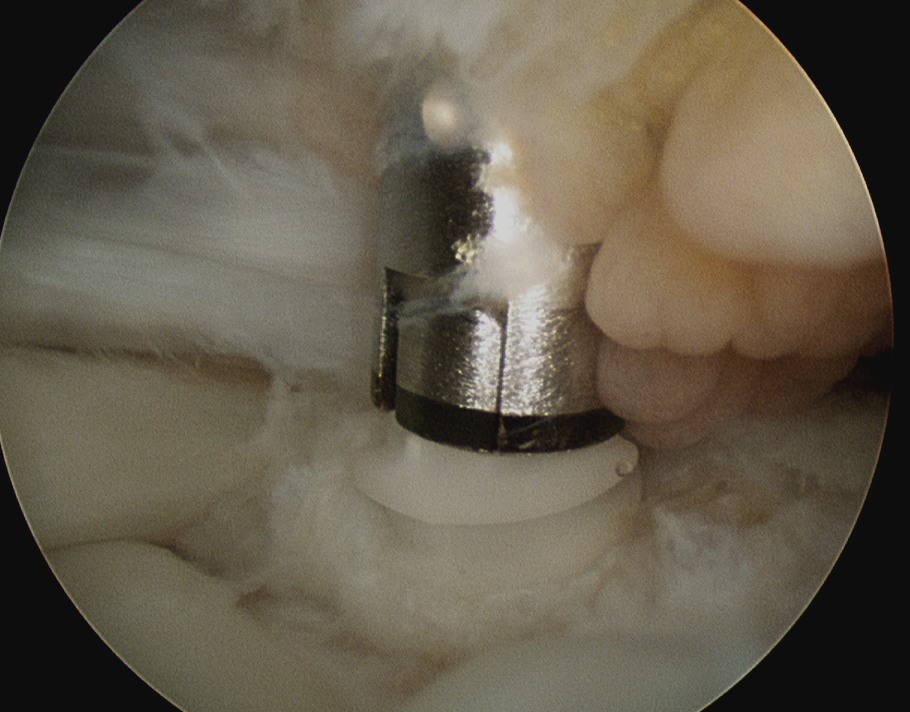
Place medial row anchors
- anterior first
- insert 18 G spinal needle and ensure good angle
- just medial to articular cartilage
- stab incision
- insert 5 mm anchor
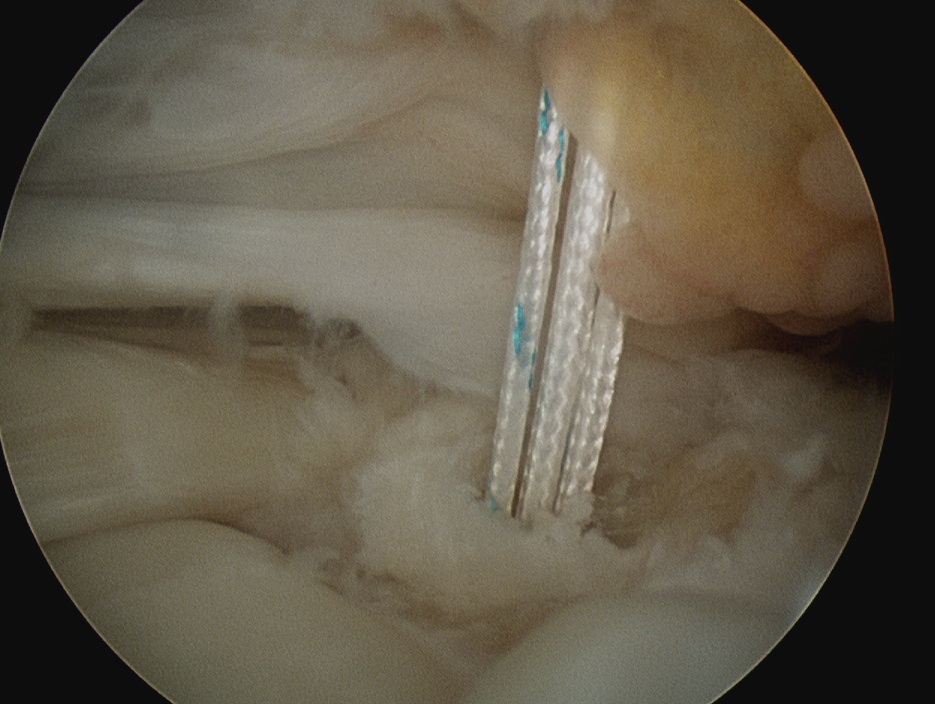
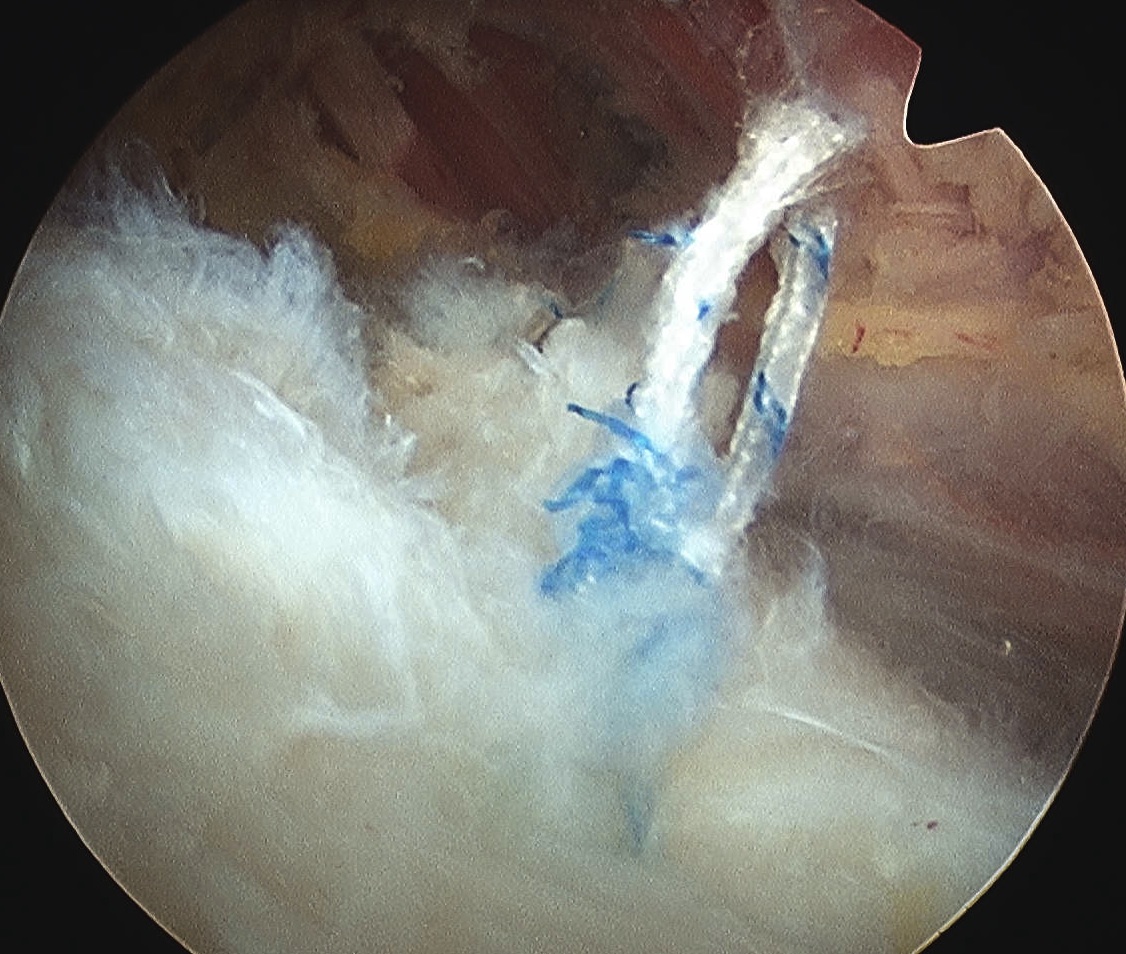
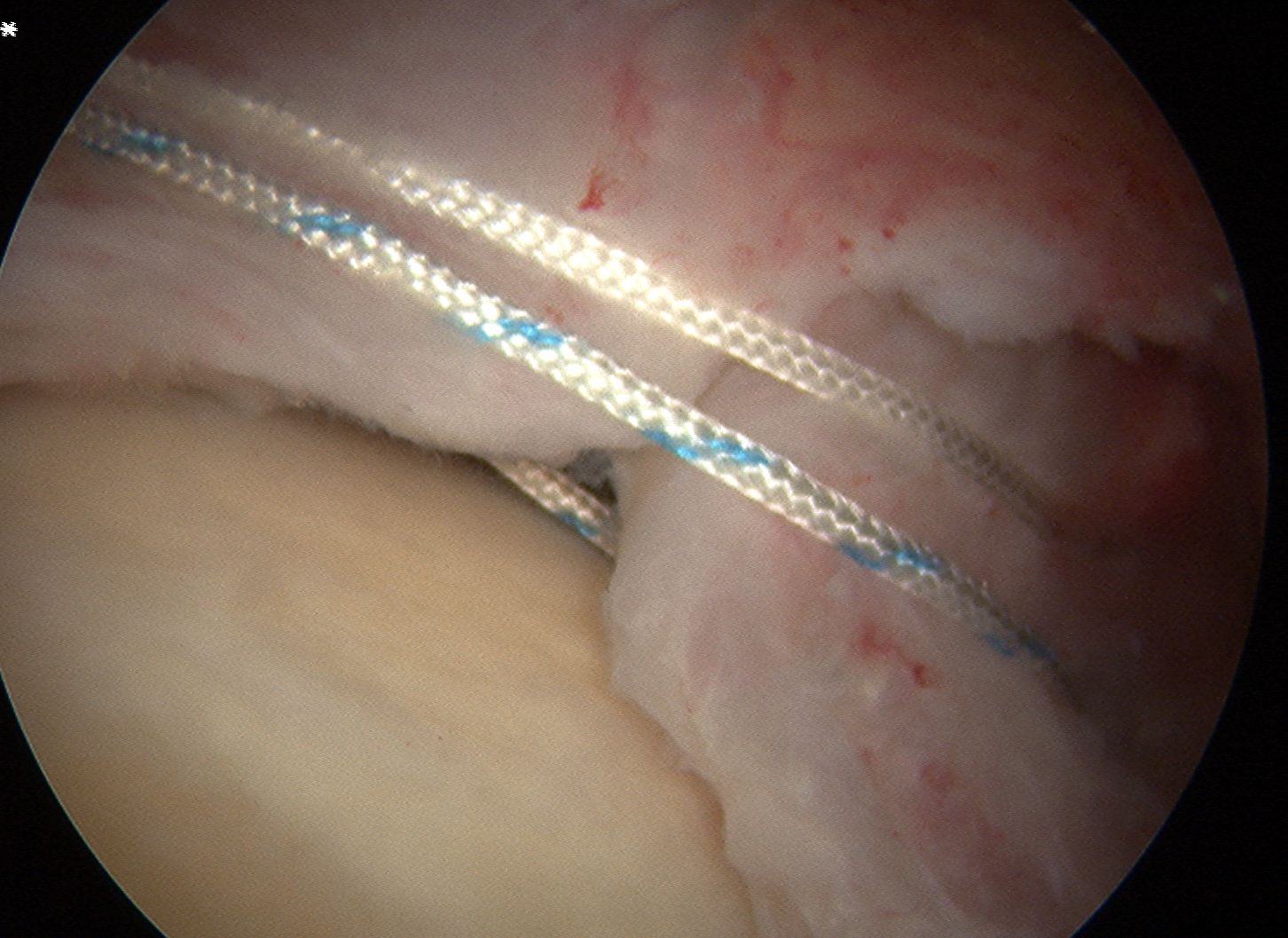
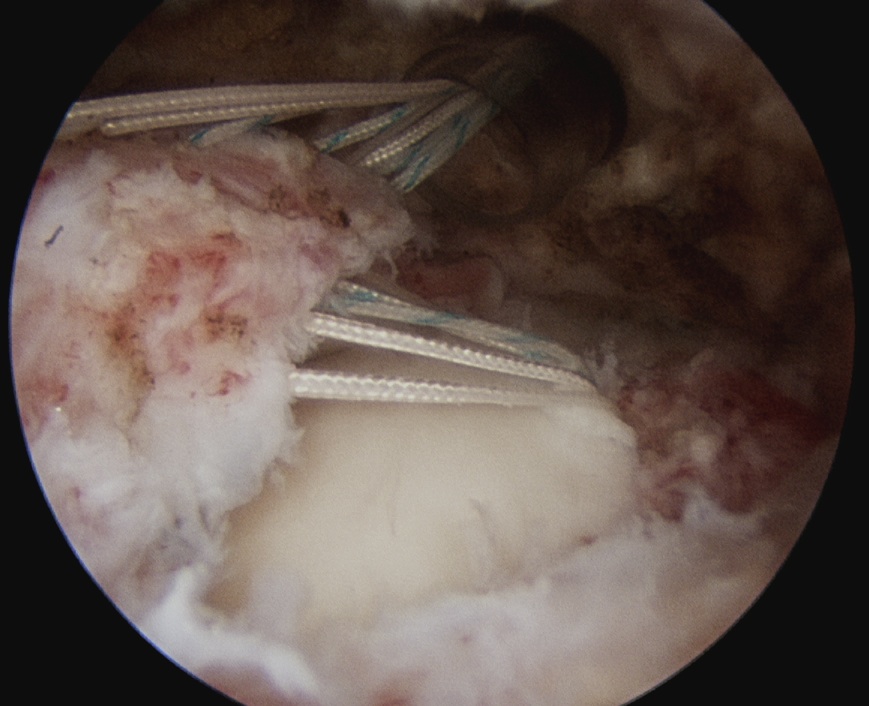
Pass sutures in lateral margin cuff
- camera posterior
- elite / scorpion / concept suture passer via lateral portal
- pass sutures through cuff anterior to posterior
- retrieve sutures through anterior portal
- retrieve via anterior portal
Repeat with posterior anchors
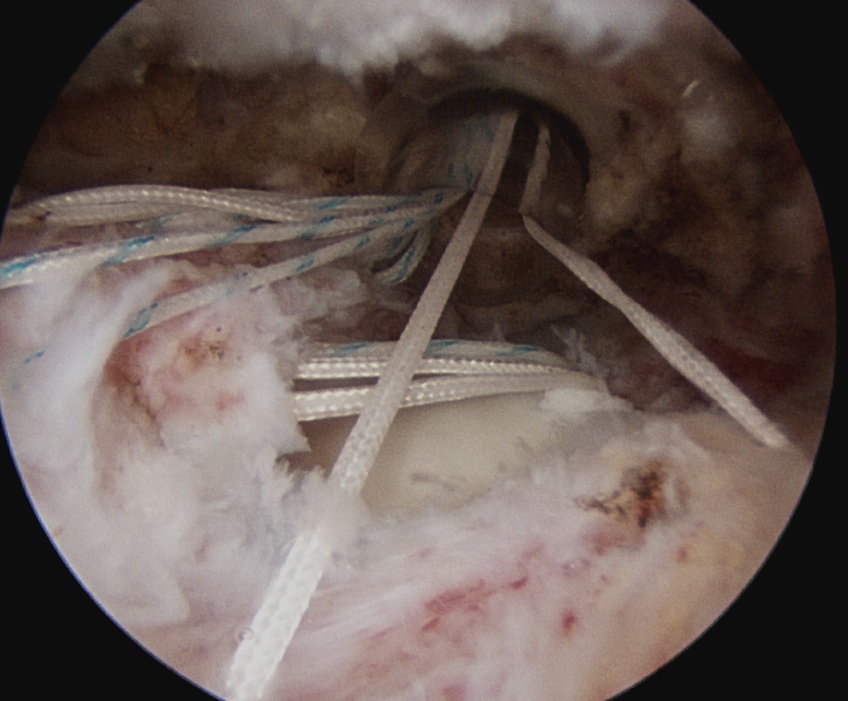
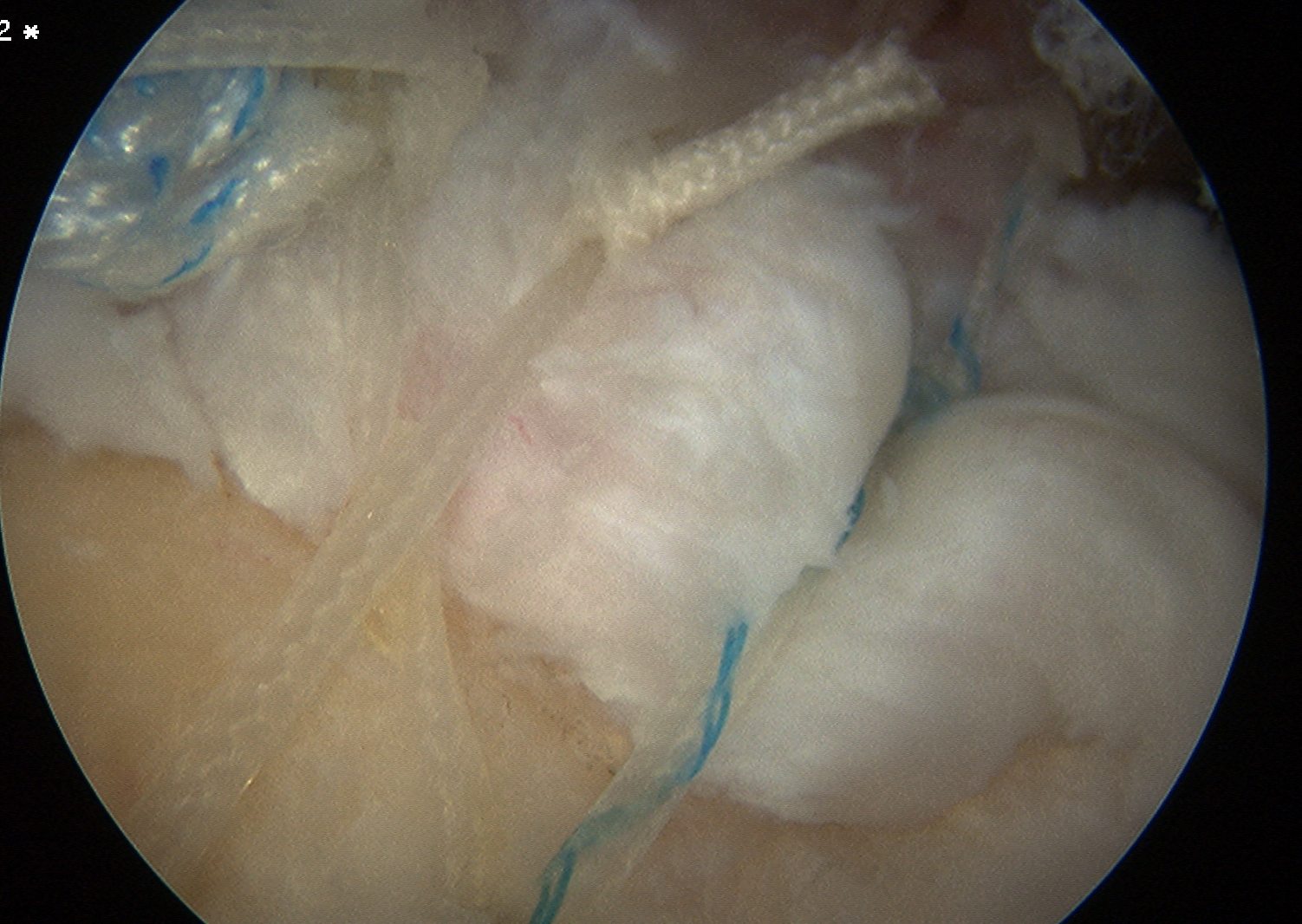
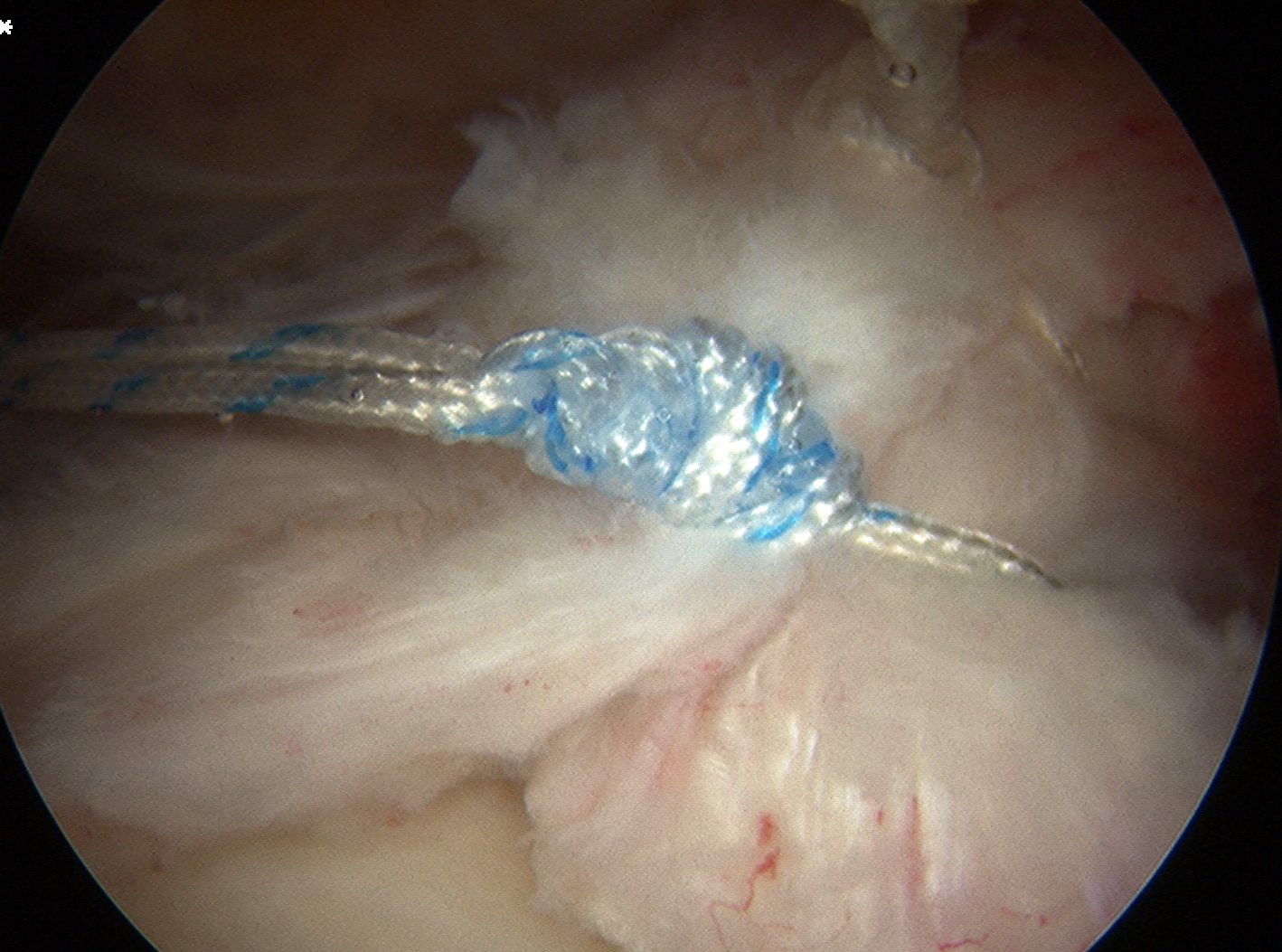
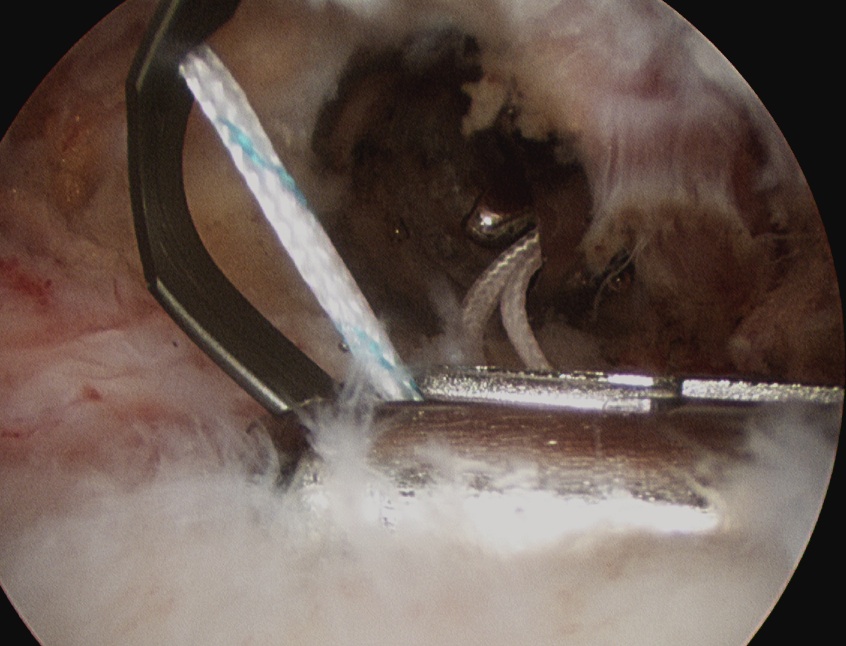
Tie sutures
- posterior to anterior / anterior to posterior
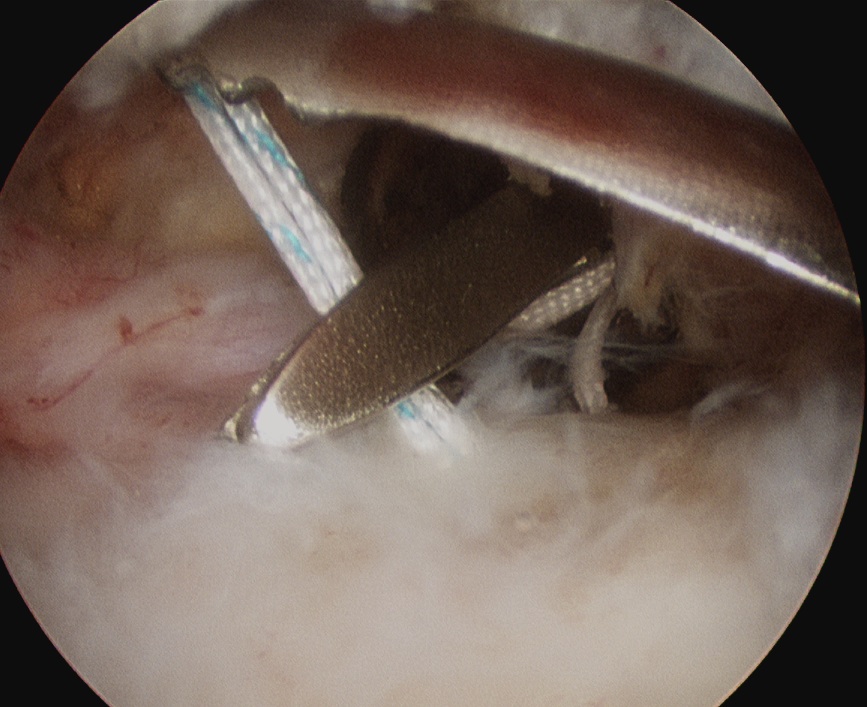
Double row
- either pass second lateral row of anchors or
- use foot print anchors, retrieve previous sutures
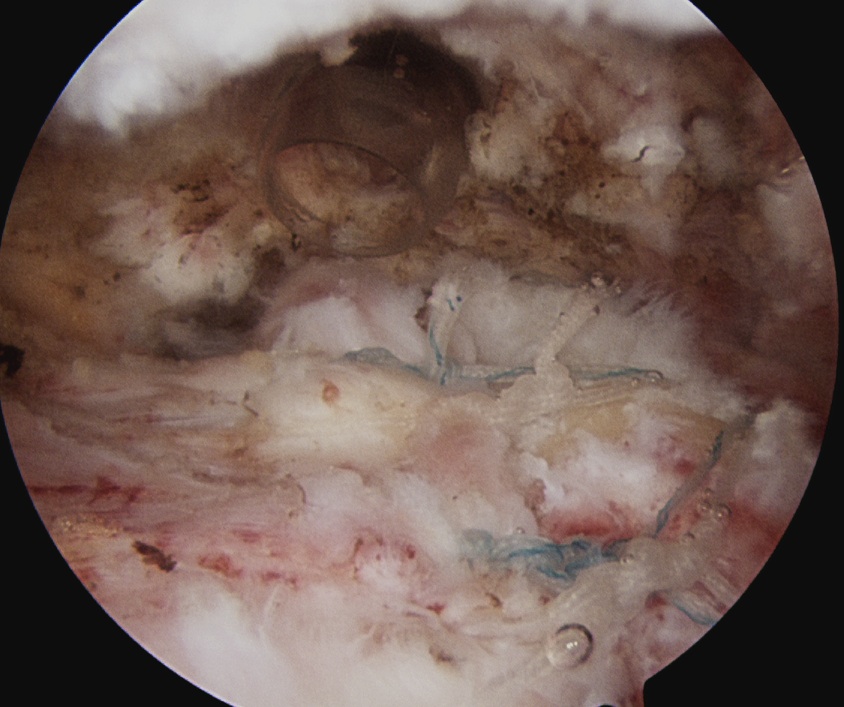
- can make suture bridge configuration
- check repair via lateral portal