Epidemiology
Dominant arm of middle aged men between 40 and 60
Kelly et al Am J Sports Med 2015
- national database study
- mean age 46
- 95% male
- increased with smoking and increased BMI
Etiology
Usually trauma related
- sporting / weightlifting injury
- resisting heavy extension load
Pathology
Degenerative changes seen on histology
Types
Complete
Retracted proximally - rupture of lacertus fibrosis
Minimally retracted
Partial
- low grade - partial tears of some fibres
- high grade - near complete avulsion of biceps tendon from radial tuberosity
History
Feel pop / tear at elbow
Lifting heavy object
May be prodromal symptoms of elbow pain
Examination
Acute onset pain / distal swelling / bruising
Reverse popeye - biceps muscle bulge proximally





Bilateral distal biceps rupture
Hook test
- attempt to hook finger about biceps tendon, from a lateral to medial direction
- can get a false positive from the lacertus if hook from medial to lateral
- unable to palpate biceps tendon

Luokkala et al, Shoulder Elbow 2020
- sensitivity in acute complete tears: 78%
- much lower in partial tears: 30%
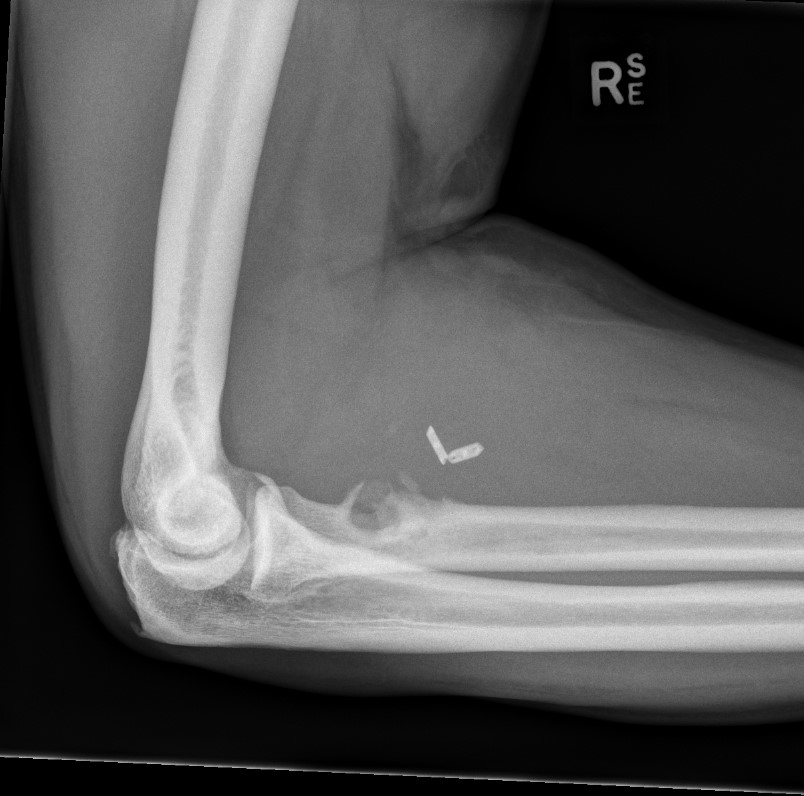
X-ray
Usually normal
Rarely see bony avulsion from radial tuberosity
Ultrasound
Simple
Can be used to confirm full thickness tears
Less reliable in partial tears
Lobo et al AJR Am J Roentgenol 2013
- ultrasound diagnosis distal biceps injury
- complete tear: sensitivity 97%, specificity 100%, accuracy 98%
MRI
Confirm diagnosis
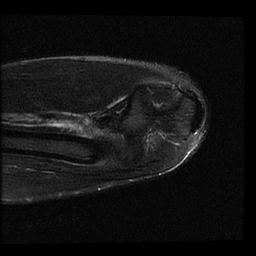
A. Complete tear / retracted
Best seen on sagittal MRI
Sagittal MRI - distal biceps retracted into arm
Sagittal MRI - distal biceps retracted into arm
Coronal MRI with 2 cm retracted distal biceps tendon
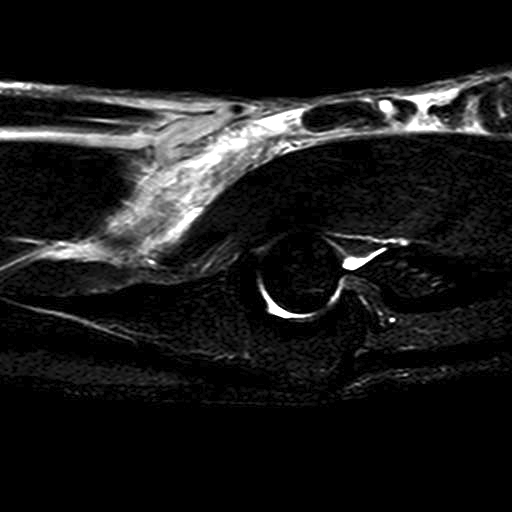
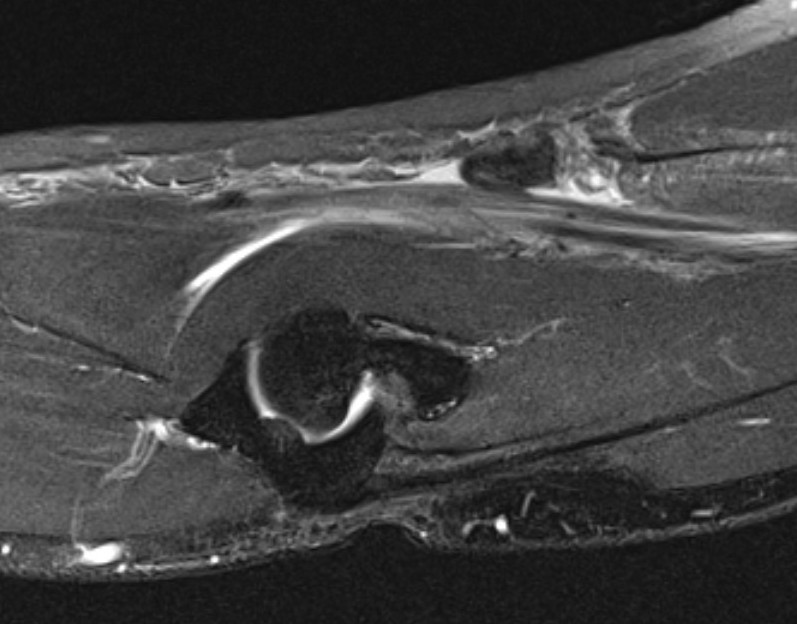
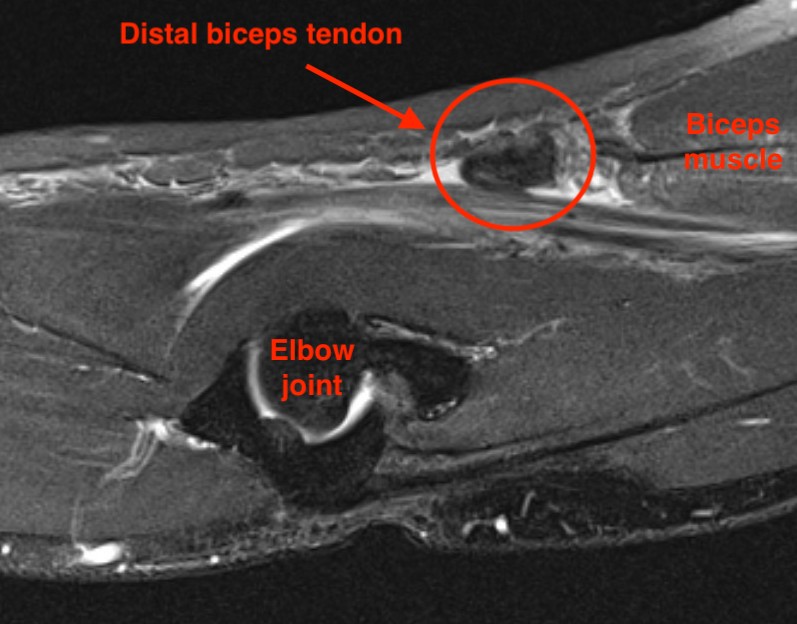
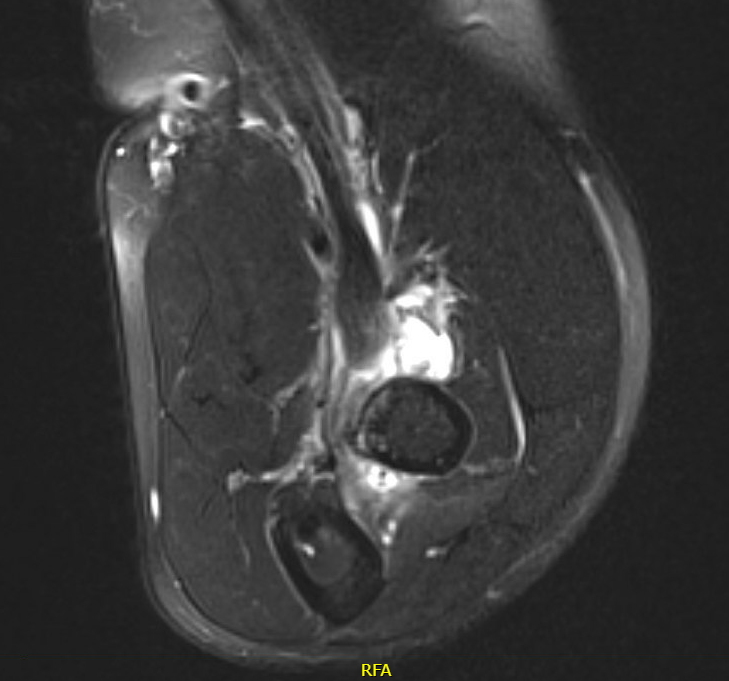
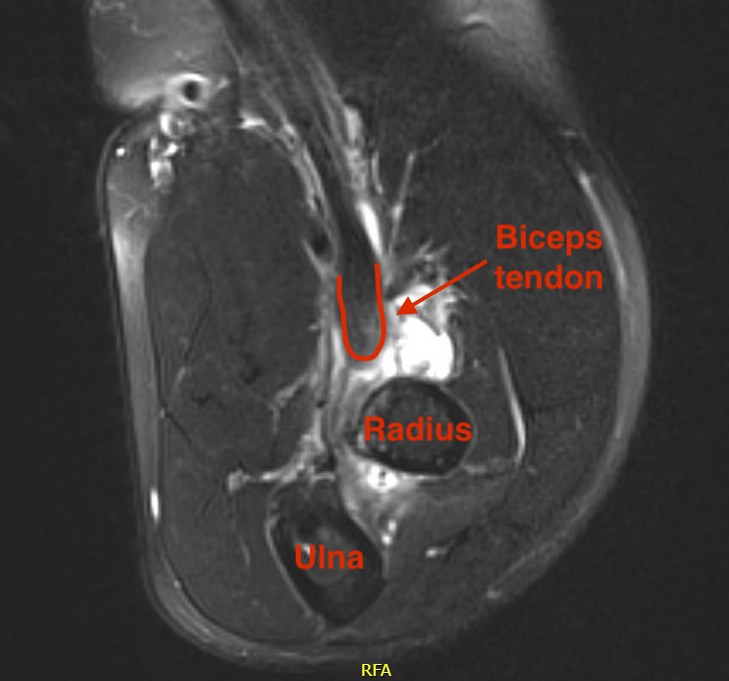
B. Partial tear
Best evaluated on the axial view
- absence of low signal intensity biceps tendon insertion onto tuberosity
- present of soft tissue edema
Management
Non-operative
Indication for complete tears
Elderly patients who do not require full strength and endurance
Chronic tears
Results
- 40% loss of supination strength
- 30% loss of flexion strength
- systematic review of operative versus nonoperative management
- 62 studies with 2481 cases
- improved flexion and supination strength with operative management
- improved flexion and supination endurance with operative management
- improved outcome scores with operative management
Operative
Indication
Young active patients with recent rupture
- may be more difficult with chronic tears
Options
One incision
- single anterior incision
- use suture anchors / endobutton to fix to tuberosity through this incision
Two incision Boyd and Anderson
- anterior incision to retrieve tendon
- posterior incision to attach tendon to radial tuberosity
Results
Single versus double incision
- RCT single incision with 2 suture anchors versus 2 incision with drill holes
- no difference in outcomes except 10% increased flexion strength with 2 incision
- increased injury to lateral cutaneous nerve of the forearm with single incision
Dunphy et al Am J Sports Med 2017
- retrospective cohort of 784 repairs
- higher posterior interosseous nerve palsy with two incision (3.4% vs 0.8%)
- higher heterotopic bone formation with two incision (7.6% vs 2.7%)
- higher reoperation with two incision (8.3% vs 2.3%)
- higher LCNF and superficial radial nerve with single incision
One incision suture anchor versus cortical button
Return to sport
- 35 NFL players with distal biceps repairs
- high rate of return to play at previous performance level
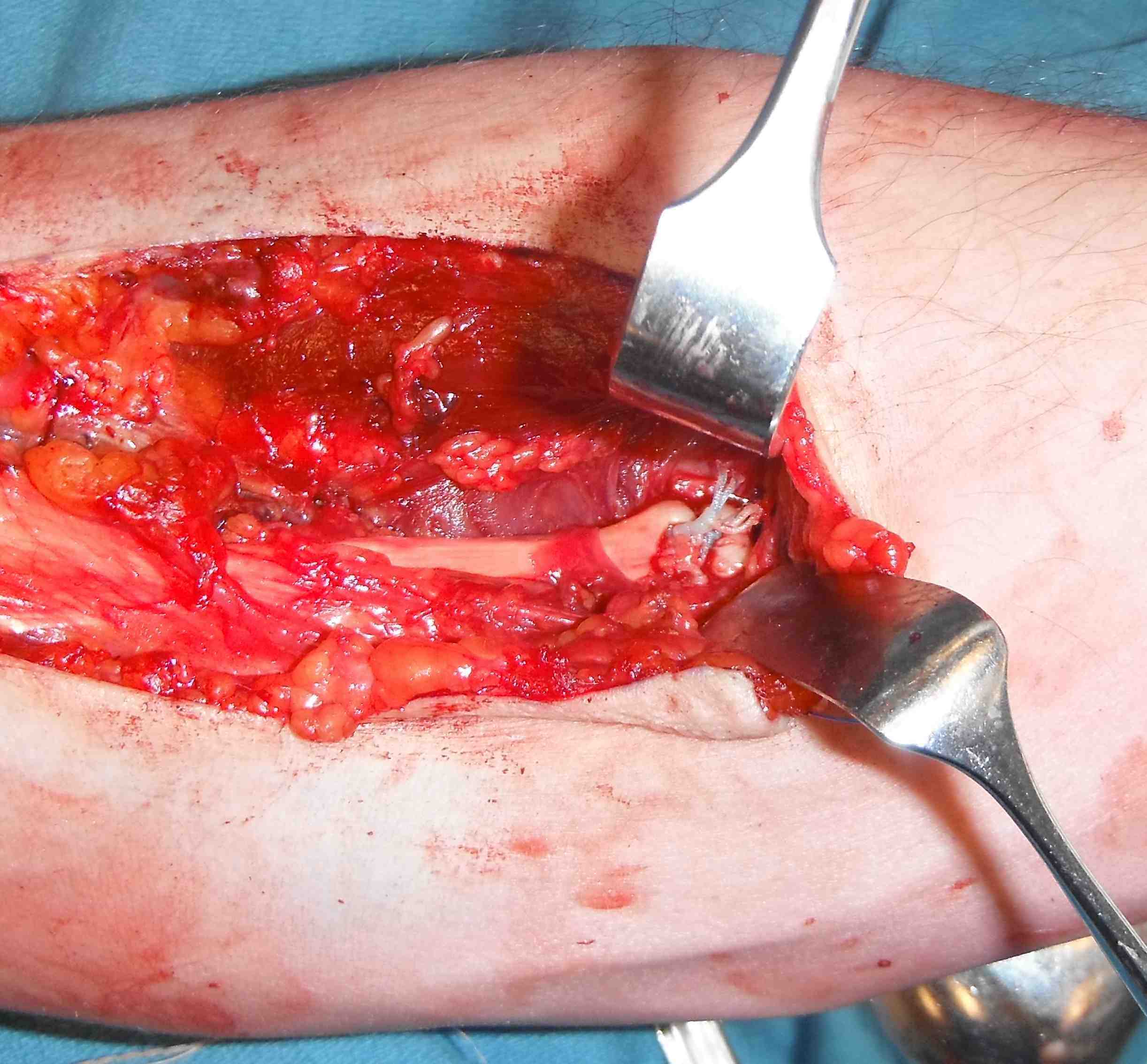
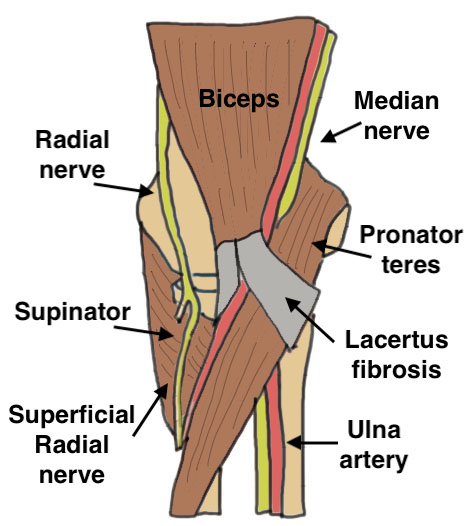
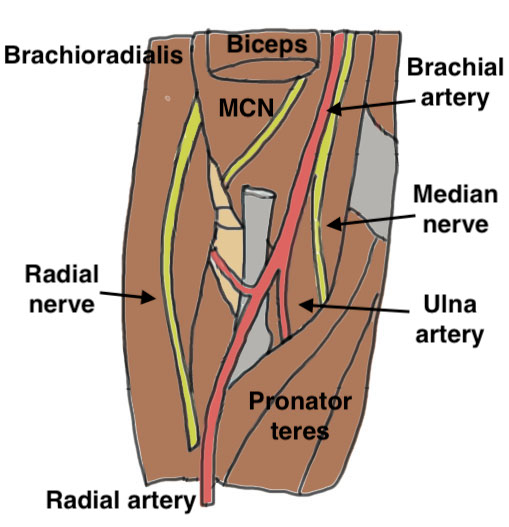
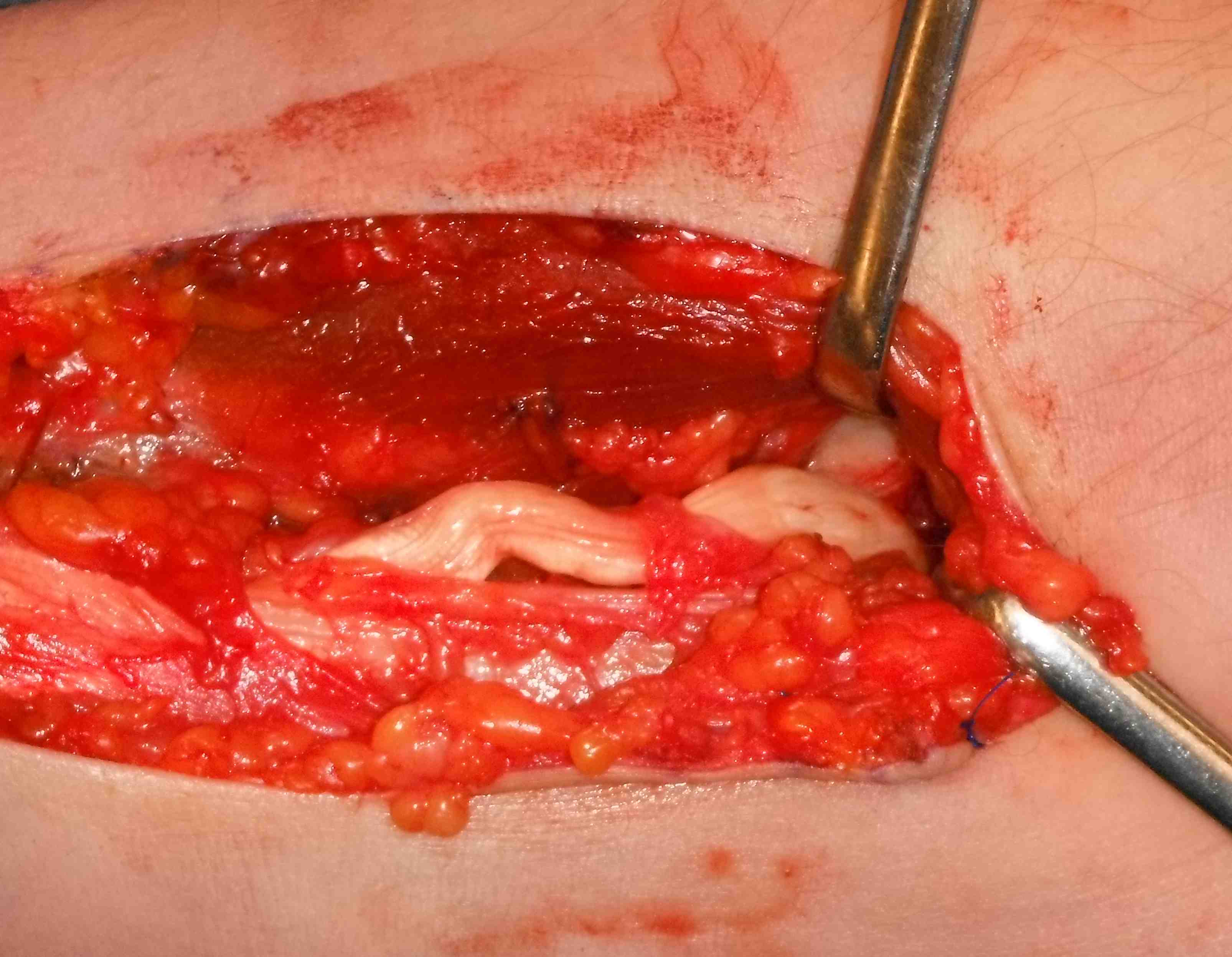
Anatomy
One incision technique with endobutton
Vumedi Arthrex Adjustable button technique
Set up
- supine, arm board, tourniquet
Incision
- proximal Henry approach to proximal radius
- protect lateral cutaneous nerve of the forearm
- divide fascia
- mobile wad medially
- divide recurrent leash if needed
- supinate forearm
- reflect supinator muscle laterally
- identify bicipital tuberosity
- can place hohmann retractors medially but not laterally as they can injure PIN
Prepare radial tuberosity
- forearm fully supinated to protect PIN
- pass guide wire through both cortices centred in tuberosity
- pass cannulated 4.5 endobutton drill
- use burr or ACL drill 8 mm to open volar cortex only to take biceps tendon
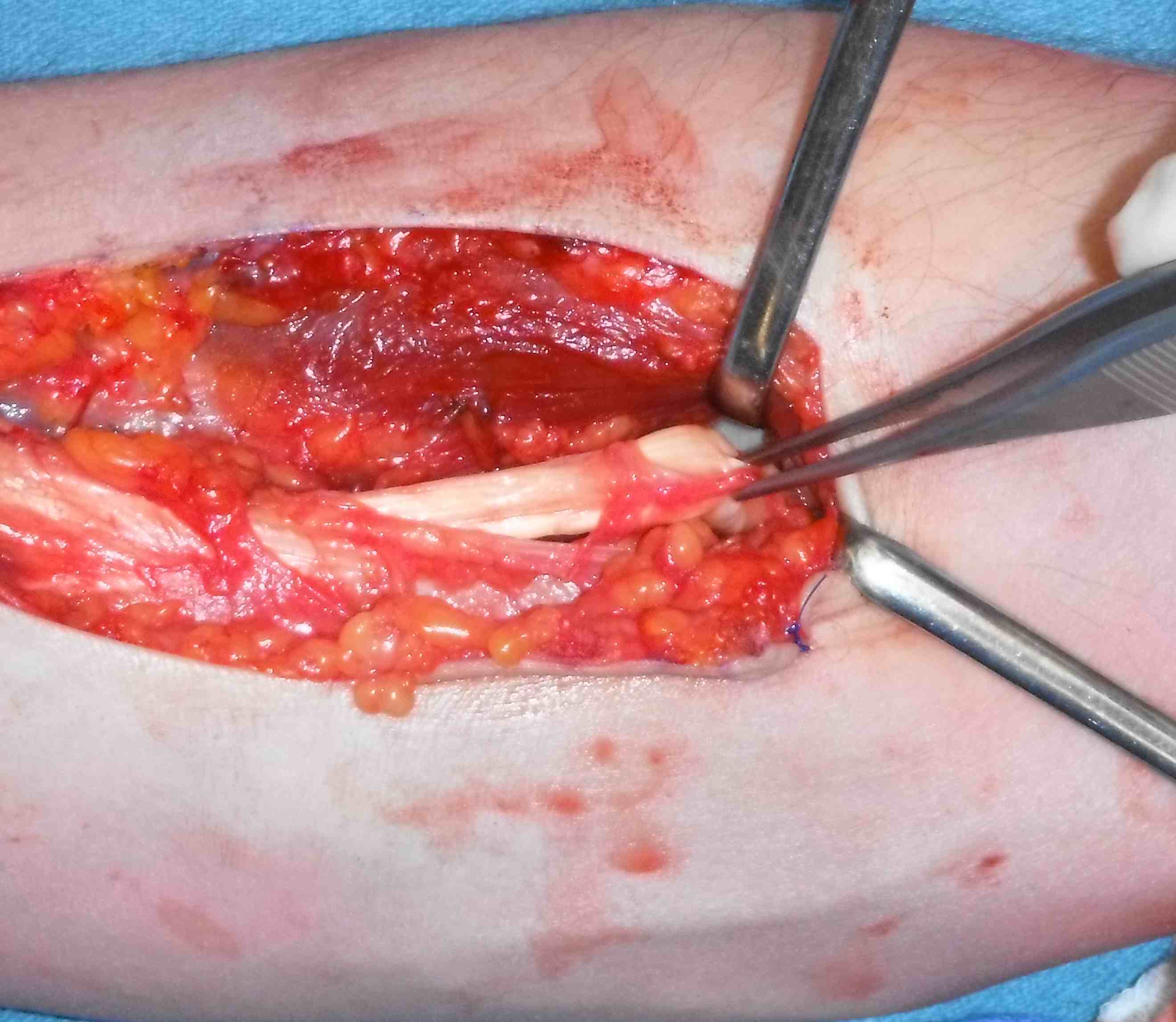
Find biceps tendon
- an additional proximal incision can help with retracted biceps
- divide fascia
- blunt dissect and deliver tendon into proximal wound
- whip stitch with high strength suture to endobutton
- enter lateral aspect tendon proximally and suture down to distal aspect
- pass around middle two holes of endobutton
- back up medial aspect and tie
- leave 2 mm space between endobutton and distal end of tendon
- allows space for dorsal cortex of radius


Tunnel distal biceps tendon to radial tuberosity
- find pathway with blunt dissection
- pass beath pin through tuberosity and skin with endobutton passing sutures
- pass and flip endobutton
- can check using image intensifier



Two incision Technique
AO surgery foundation technique
Technique
Anterior
- Henry approach
- maximally pronate forearm
- hug border of radius with curved hemostat
- avoid periosteum of ulna to prevent synostosis
- palpate tip dorsally in extensor mass
- dissect down to radius
Posterior
- Thompson's approach
- line from lateral epicondyle to lister's tubercle
- between EDC and ECU
- expose and split supinator
Repair
- performed through bone tunnels
Post operative management
- RCT of early mobilization versus 6 weeks immobilization
- 83 patients treated with suture button followed for 12 months
- trend towards better ROM with early mobilization
- better QuickDASH scores over time with early mobilization
Partial Tears
- 74 patients with partial distal biceps tears
- 34/61 (55%) treated nonoperatively went on to have surgery
- high grade partial tears (>50%) on MRI more likely to need surgery
Chronic Tears
Issue
> 3 weeks old
- harder to repair
- associated with higher complication rates
- have to repair in significant position of flexion
> 6 - 8 weeks
- tendon involutes into biceps
- need either hamstring autograft or allograft reconstruction
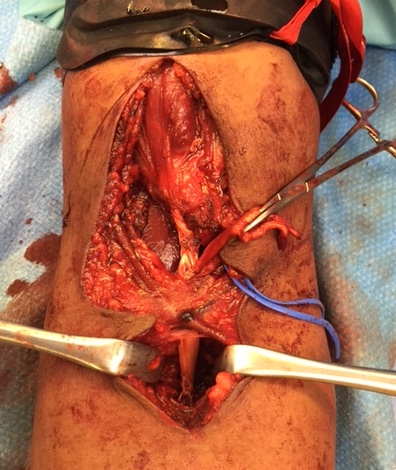
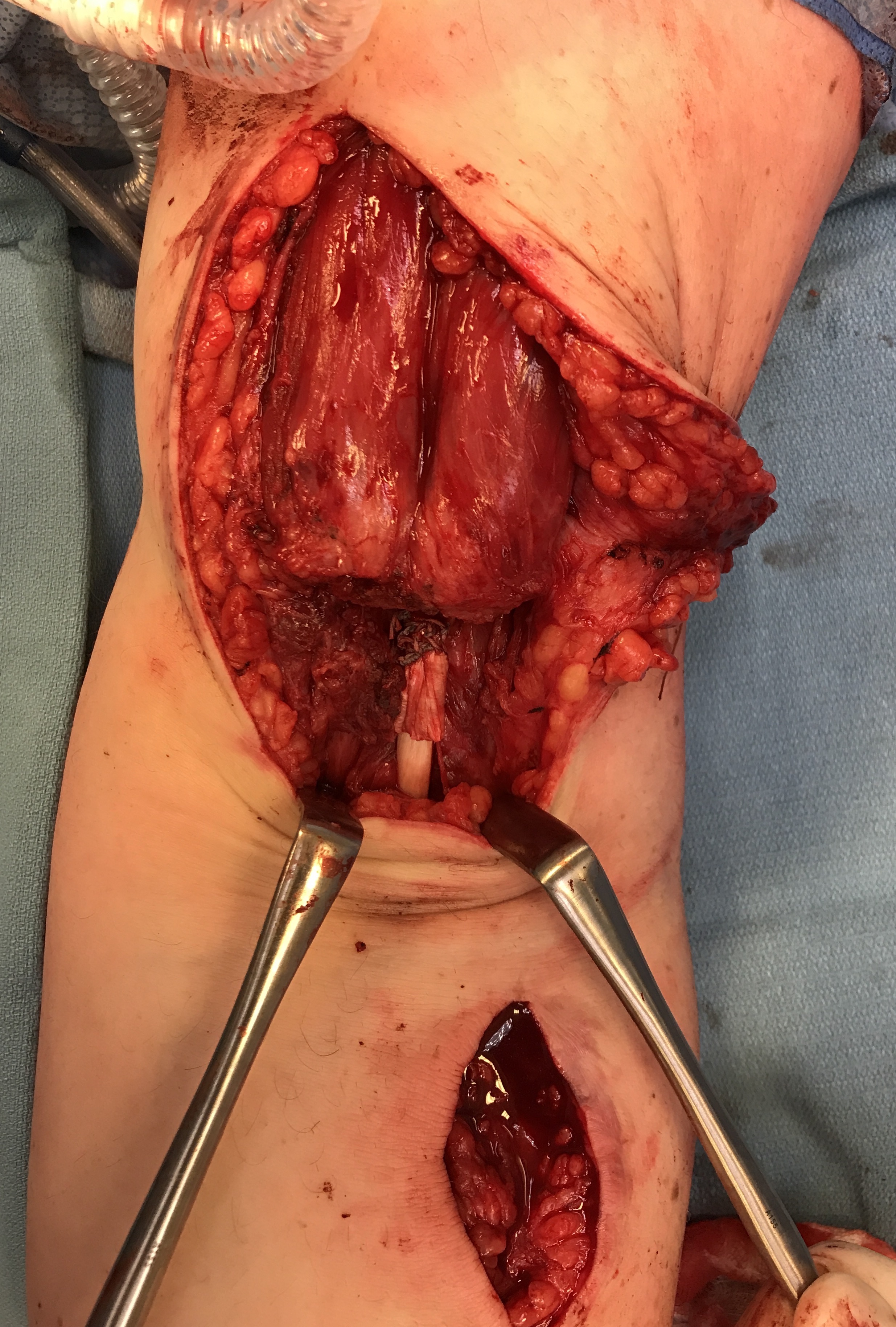
Technique
Vumedi allograft distal biceps reconstruction
Incision
- S shaped, proximal medial and lateral distal
- identify and protect the brachial artery and medial nerve in the proximal approach
- identify the radial tuberosity through the lateral distal approach

Graft options
Hamstring allograft
Tibialis anterior or posterior allograft
Tendoachilles allograft with bone block removed
Technique
Secure to radial tuberosity with endobutton first
- approach and mobilize biceps muscle
- brachial artery is directly medial
- then weave graft through distal biceps muscle belly
- pulvertaft
Results
- compared 46 allograft distal biceps reconstructions to primary repair
- no difference in functional outcome at mean 5 years
Complications of distal biceps repair
Amarasooriya et al Am J Sports Med 2020
- systematic review of complications after distal biceps repair
- 1.6% PIN injury
- 1.4% median nerve injury
- 1.4% re-rupture
- 9.2% lateral cutaneous nerve injury
- 0.1% synostosis / brachial artery injury / compartment syndrome / radial fracture
PIN Palsy
- 230 patients
- 3.2% developed postoperative PIN palsy
- all 9 resolved at average of 86 days (range, 41 - 145)
Reichert et al Med Sci Monit 2018
- 7 cases of PIN palsy with no recovery after 3 months
- 5 demonstrated nerve entrapment by scar or by biceps
- 2 demonstrated PIN division secondary to drill
Failure fixation