Aetiology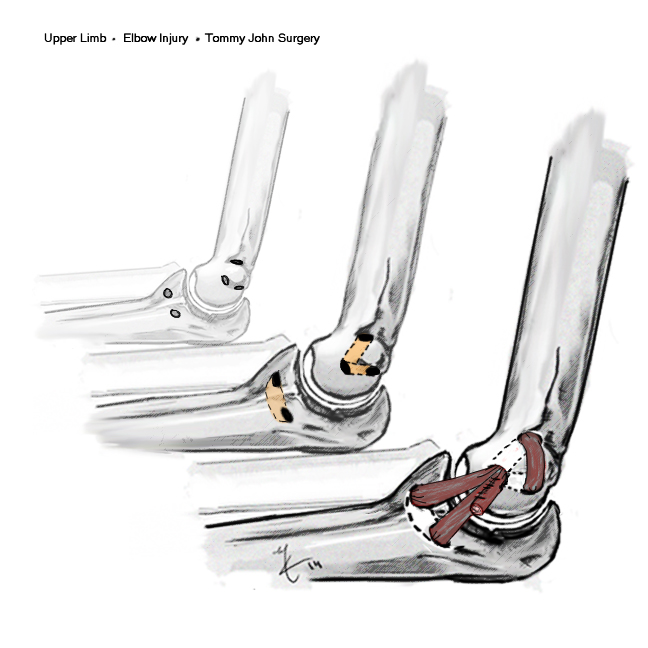
Throwing injury
- seen in the throwing athlete
- repetitive microtrauma / valgus stress
- develop laxity
Little leaguer's elbow
History
Initially
- lose velocity / accuracy
Develop medial pain
40% ulna nerve symptoms
Examination
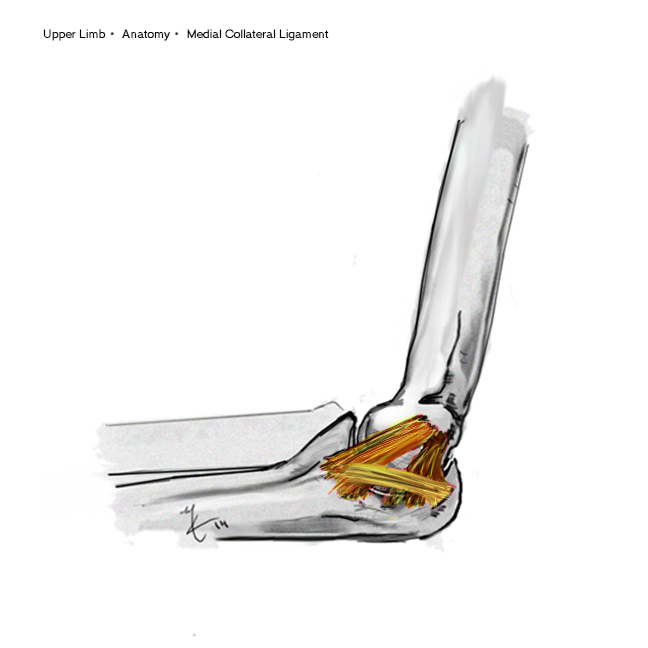
Pain on palpation of anterior bundle MCL
CFO muscle bulk covers insertion in full extension
- reveal UCL with flexion
Jobes test
Valgus stress with elbow flexed 25o to unlock olecranon
- forearm pronated to prevent false positives due to lateral side laxity
- problem is shoulder ER
Modification
- lie patient prone
- apply valgus stress


Milker test
- shoulder ER
- thumb pointing out
- extend arm whilst placing valgus strain


Anatomy
X-rays
40% calcification MCL
Stress view
- > 3mm difference from opposite side
MRI
Nearly all throwing athletes / pitchers will have abnormalities
- don't decide surgery on basis of MRI findings
Management
Non Operative
RICE
NSAIDS
Physio
- may be muscle imbalance in throwers
- overactivity of EDC and ECRB aggravates valgus
- physio to balance flexors and extensors
- radial deviators vs Ulna deviators
- if doesn't settle consider reconstruction
Really amounts to 6/12 rest
- problem for professional athletes
Operative
Tommy John Surgery
Named after famous American baseball pitcher
- first to have this surgery
Options
1. Repair
- not often able to be done
- perhaps in acute tear
2. Reconstruction with free graft
+ / - transpose ulnar nerve anteriorly out of the way
- many techniques described
UCL reconstruction
Numerus techniques described
Palmaris longus / gracilis graft
Ulna tunnel
- proximal ulna at level coronoid tubercle
- AP
Humeral tunnel
- medial epicondyle
- Y shaped
- no posterior cortical penetration to avoid injury ulna nerve
Figure of 8
- tension at 30o
- suture both limbs together to improve tension
Post-Op
Immobilise for 10/7
ROM brace for 4/52
No throwing for 6/12
No sport for 12/12
Results
Jimmy Andrews et al Am J Sports Med 2010
- modification Jobe technique + subcutaneous ulna nerve transfer
- 942 patients followed up for 2 years minimum
- 83% returned to previous level of sport
- returned to throwing at 4 - 5 months
- return to full sport at 12 months
Posterior Elbow Impingement
Symptoms
Cause posteromedial pain
- probably related to subtle UCL instability
May be protective
Examination
Pain posteromedially with full extension
CT
Identify posterior olecranon osteophytes
Management
Arthroscopic Resection
Maximum 2 - 3 mm
- if remove too much arthroscopically
- high incidence of UCL tear
- probably protective