Definition
A localised defect in the cortex of the metaphysis
- failure of bone to form
- skeletally-immature adolescents
Fibrous cortical defect
- < 2cm in diameter
Non ossifying fibroma (NOF)
- > 2cm
Epidemiology
Most common skeletal lesion
- 30% of young children
- most common cause of pathological fracture in children
Multiple NOF
- Neurofibromatosis 1
Location
Distal femur
Distal tibia
Goldin et al J Child Orthop 2017
- 68 NOF of the femur
- 60% medial at origin of medial head of gastrocneumius or adductor magnus
- 40% lateral at the origin of the lateral head of gastrocnemius
Muzykewicz et al J Child Orthop 2017
- 48 distal tibia NOF
- 96% distal lateral tibia
- in direct communication distal interosseous membrane
Natural history
Self limiting
- usually ossify by early adulthood
- move further from physis as growth occurs
- ? become bone islands
Fracture risk if large

Stages
Ritschl et al Skeletal Radiol 1988
- stage A: eccentric lesion near physis
- stage B: lesion with thin sclerotic margin, further from physis
- stage C: increasing sclerosis
- stage D: complete sclerosis
Clinical
Child
- incidental finding
- pain if large
- pathological fracture
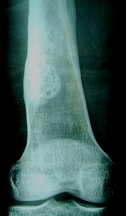
X-ray
Solitary, eccentric lytic lesion
Fibrous Cortical Defect
- < 2 cm
- small cortical lucency
- sharply defined border
Non-Ossifying Fibroma (NOF)
- > 2 cm
- eccentric metaphyseal lesion
- sclerotic margin
- slight expansion of cortex
- usually < 1/3 diameter of bone
Differential diagnosis
Unicameral bone cyst
Aneurysmal bone cyst
Pathology
Biopsy usually not necessary
Fibroblasts proliferation with multinucleated giant cells
- no bone formation
Fracture risk
Herget et al BMC Musculoskeletal Disord 2016
- 87 patients with 103 NOF
- 89% asymptomatic and incidental findings
- 10 patients symptomatic
- 6/10 symptomatic patients had a fracture
- all had bone diameter involvement 75% or more
Goldin et al J Paediatr Orthop 2020
- 32 patients with NOF of the tibia
- measured > 50% involvement sagittal and coronal, cortical breach and no neocortex
- those with all 4 risk factors had 100% fracture risk
Management
Observation
Small defects
Asymptomatic
Incidental finding
Curettage and Bone graft
Indication
- large lesions > 1/2 diameter of bone
- symptomatic
- significant cortical thinning
Results
Andreacchio et al Eur J Orthop Surg Traumatol
- 9 patients with symptomatic NOF mean age 10 years
- average size > 2/3 diameter bone
- curette and graft with Calcium Sulphate bone substitute
- all 9 healed
Pathological fracture
Management
1. Nonoperatively
- fracture heals in normal length of time
- lesion may heal with fracture union
2. Operative management
- failure to obtain or maintain an adequate reduction
2. Persistent post fracture
- curettage and bone graft