Indications for Repair
Only 20% repairable
1. Red / Red longitudinal tear
- outer 3mm / meniscocapsular junction

2. Red / White longitudinal tear
- only one side of tear vascularised

3. Young patient
Contraindications to repair
1. White / White
2. Complex / Horizontal / Radial / Degenerative tears
3. Tears that are stable & < 1 cm
4. Meniscal tear in setting of torn ACL that is not being reconstructed
- high risk of re-tearing meniscus if knee unstable
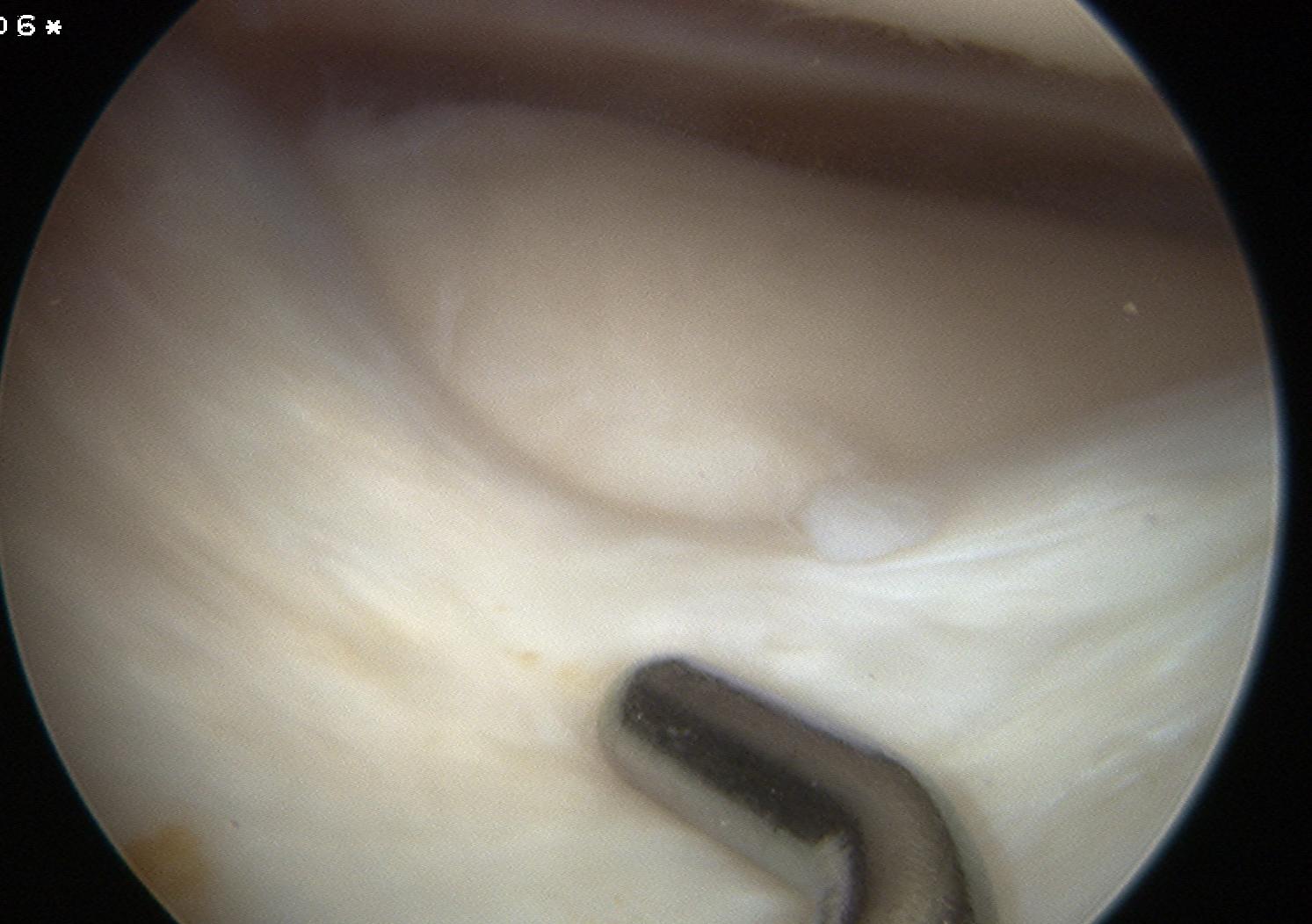
Principles of Repair
1. Debride tear
- stimulate proliferative response
- remove mature scar
- with shaver / rasp
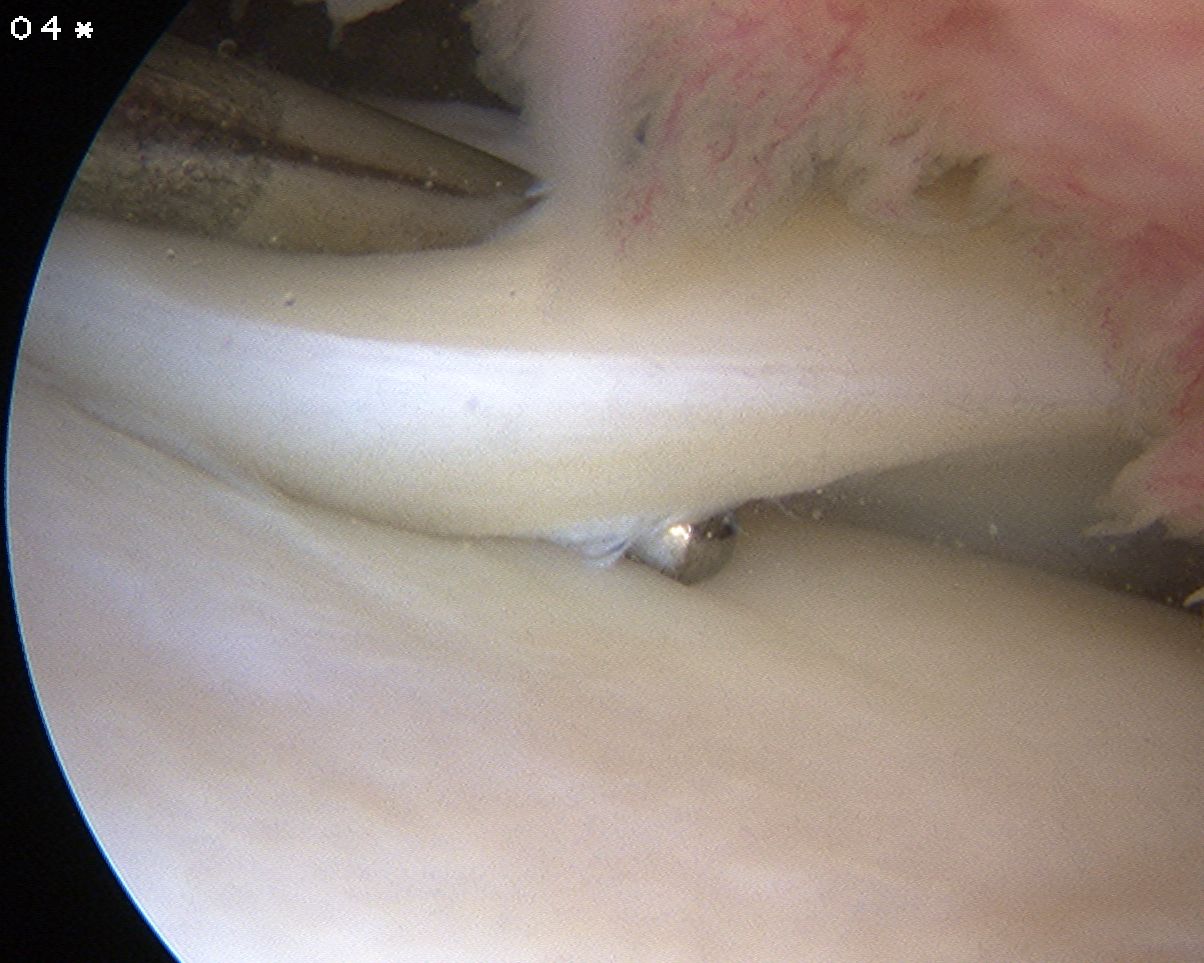
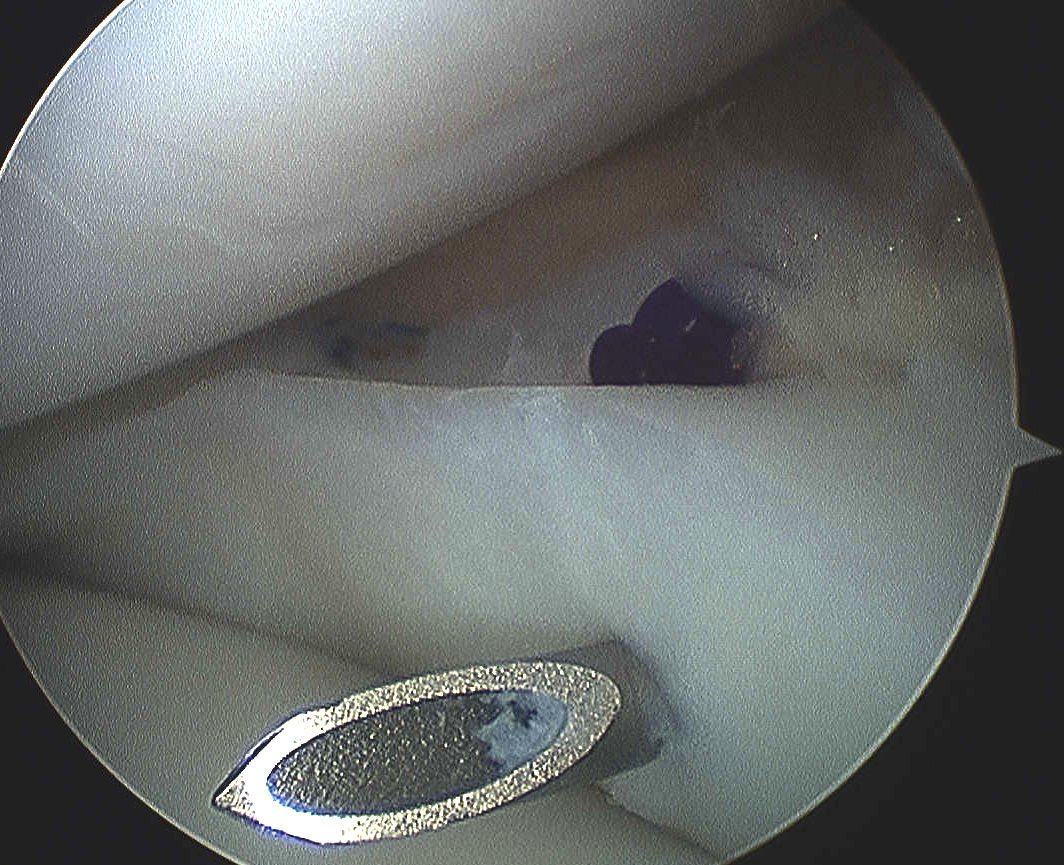
2. Trephine meniscocapsular periphery
- with spinal needle to promote vascular channels
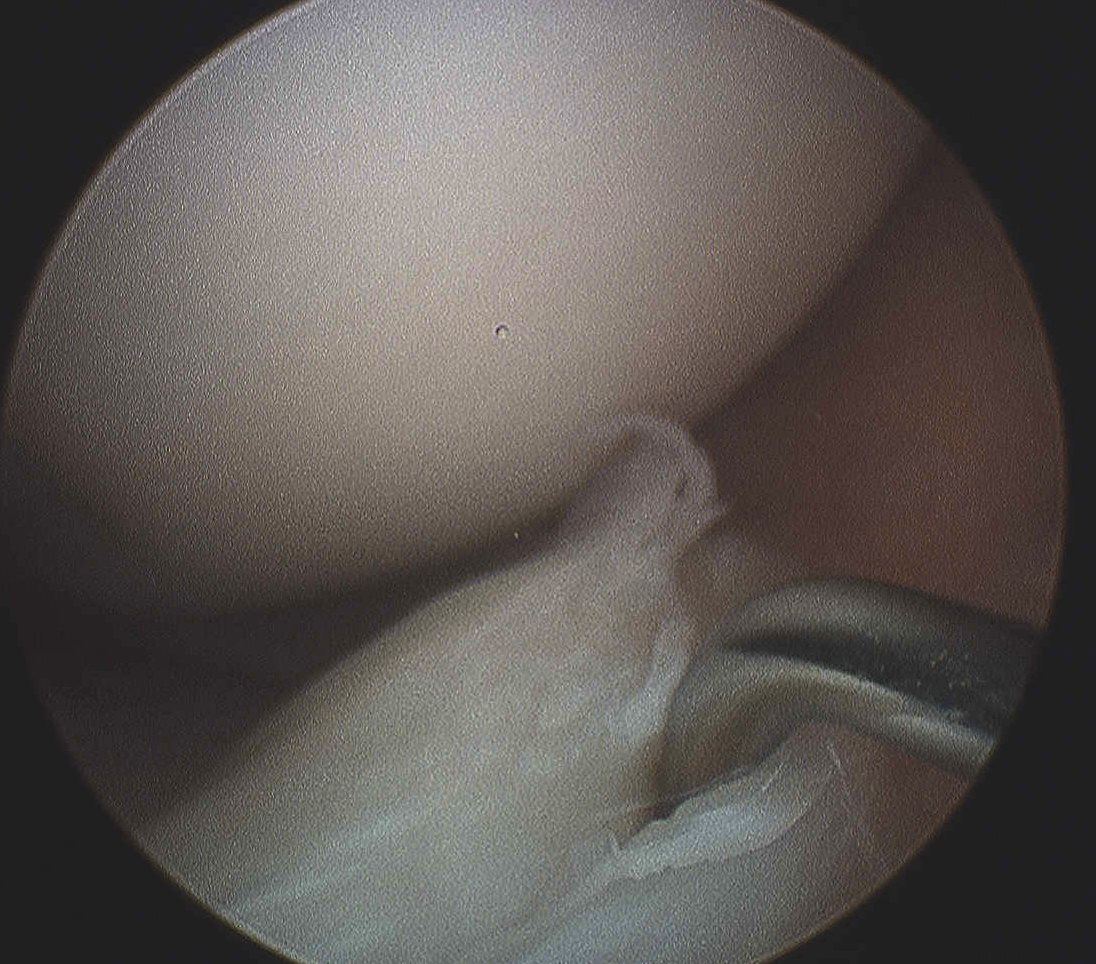
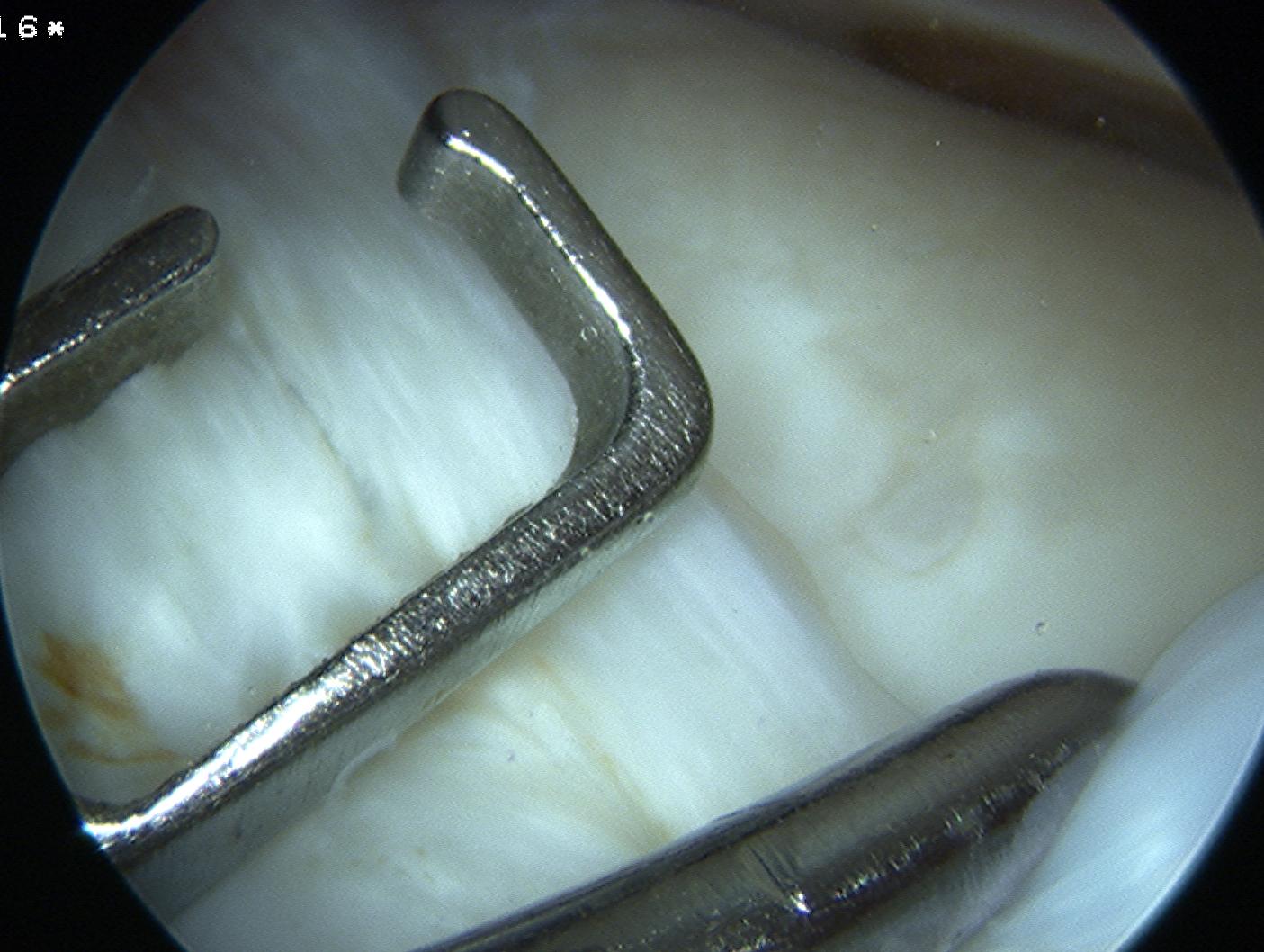
3. Reduce mensical tear
4. Suture placement
A. Open repair
B. Inside out
C. All inside
D. Outside in
5. Increase chance of healing in isolated mensical repair
- fibrin clot
- intercondylar notch microfracture
Techniques
1. Open repair
Tibial plateau ORIF
- common to need to repair capsular avulsion of LM
- repair with 4.0 PDS / ethibond
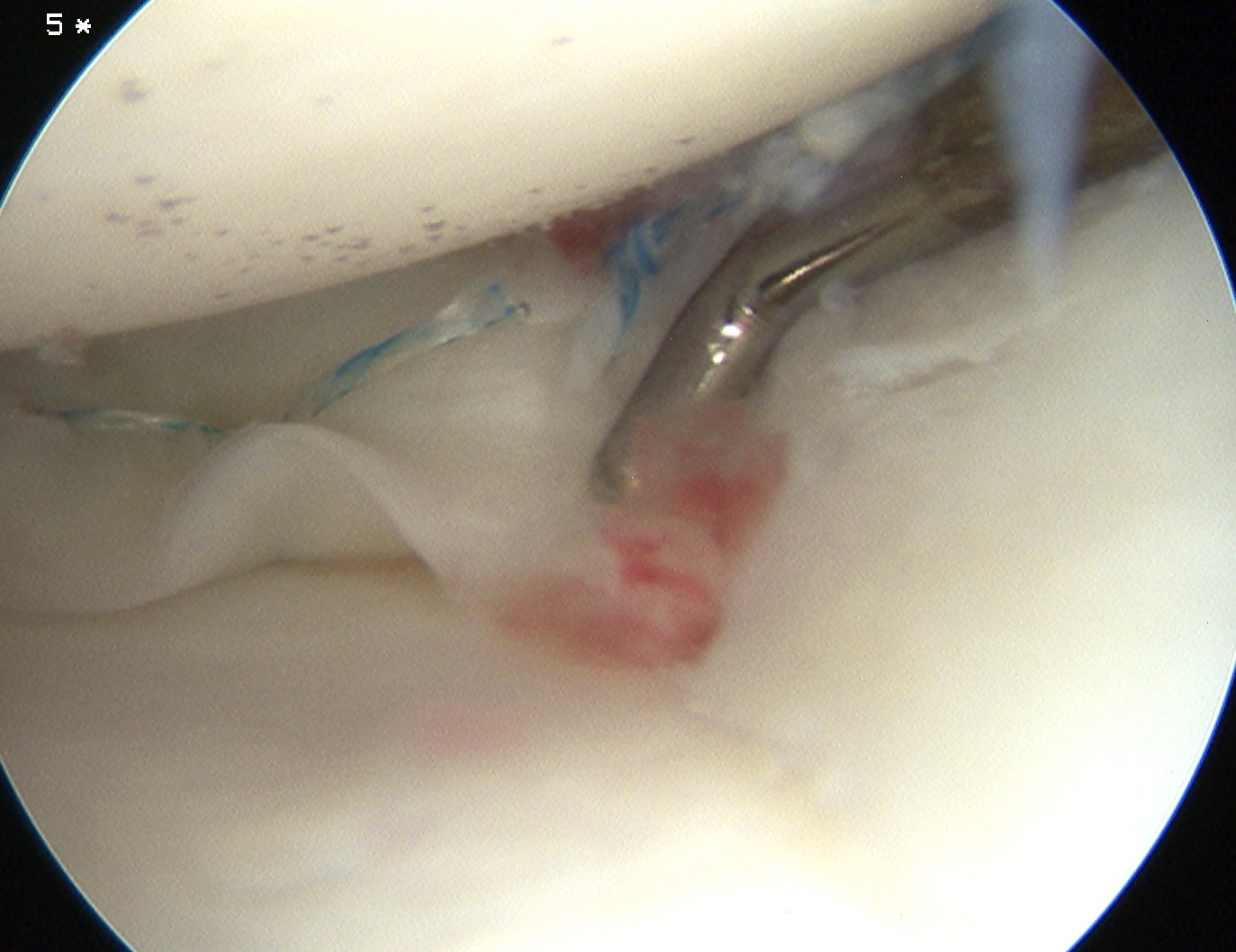
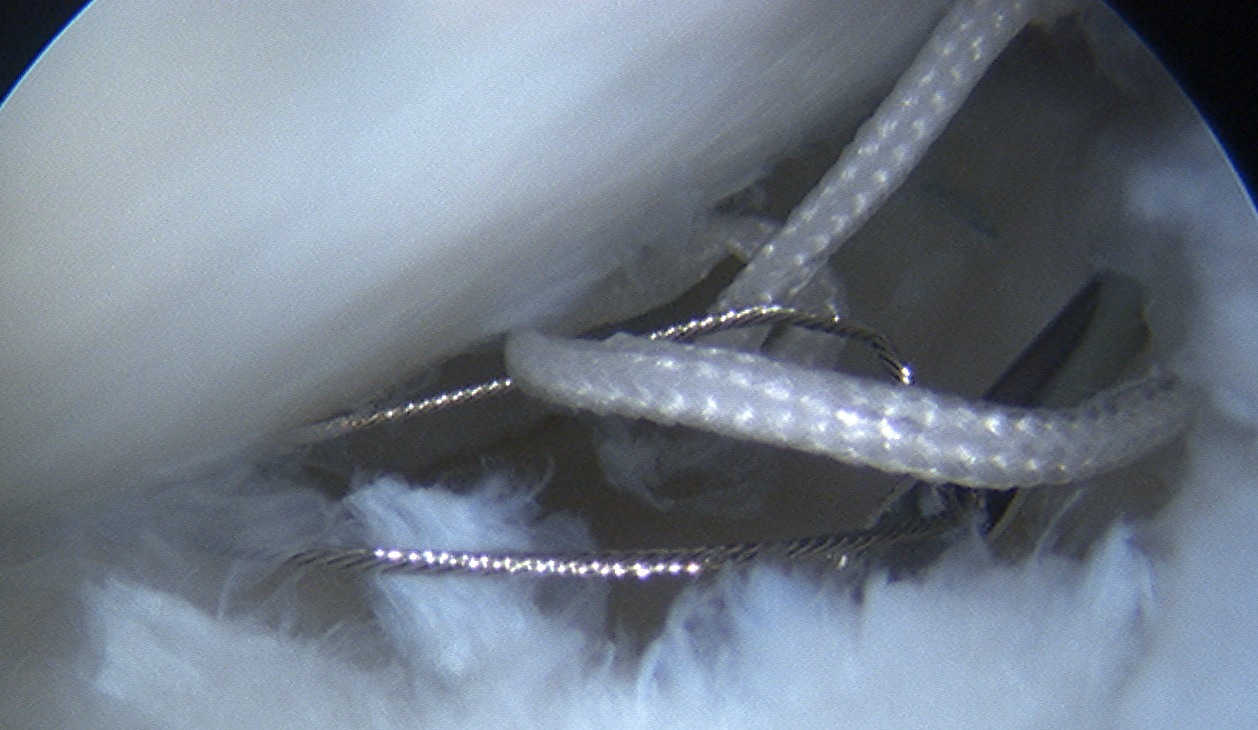
2. Inside out
Technique
Require
- double armed sutures with long flexible needles
- use single or double cannula system
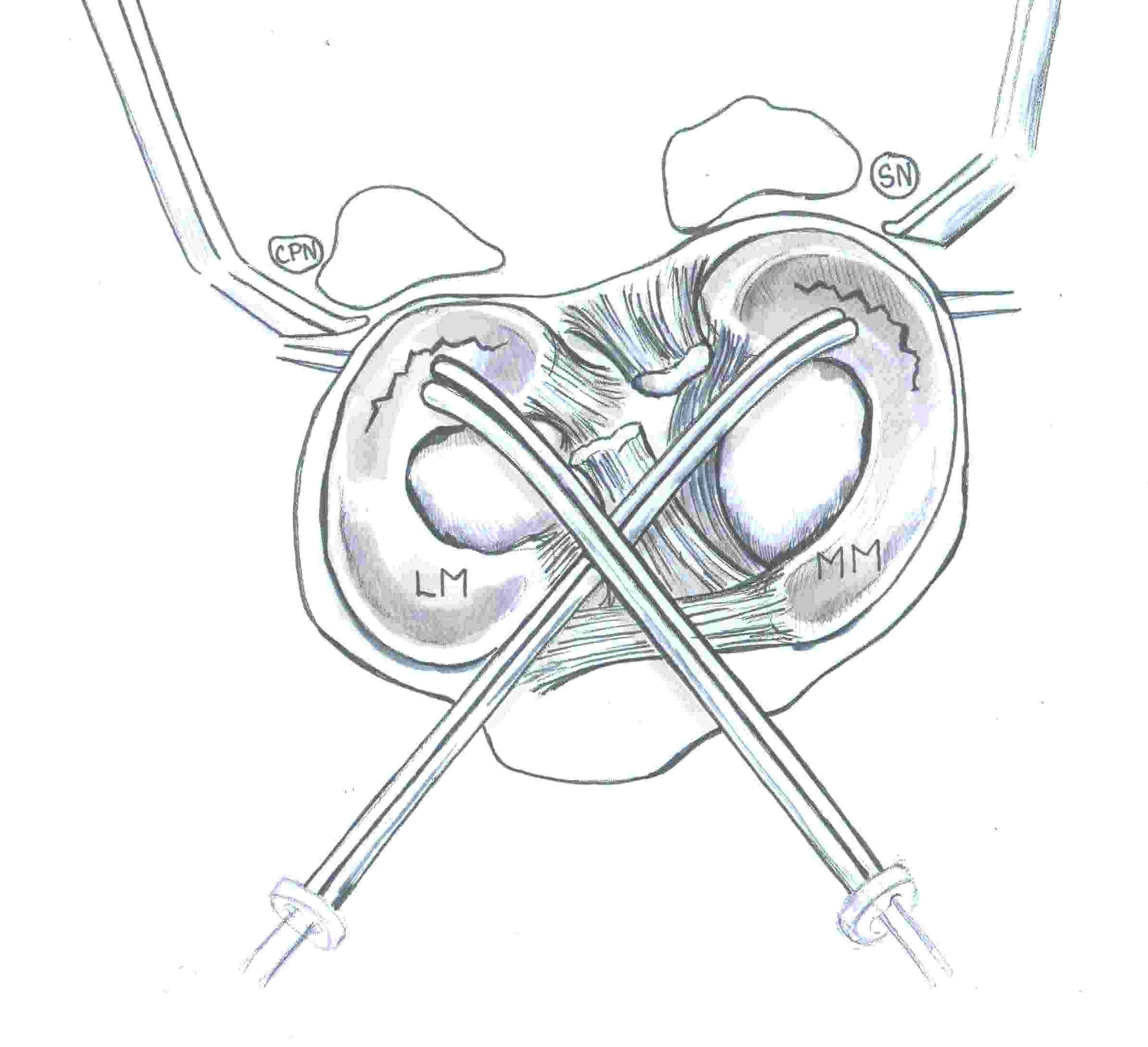
Make open posteromedial / posterolateral approach
- retrieve the sutures needles as they exit the joint capsule
- protects neurological structures (saphenous / CPN) from needle or suture injury
- sutures then tied over capsule
- pass in flexion to protect structures
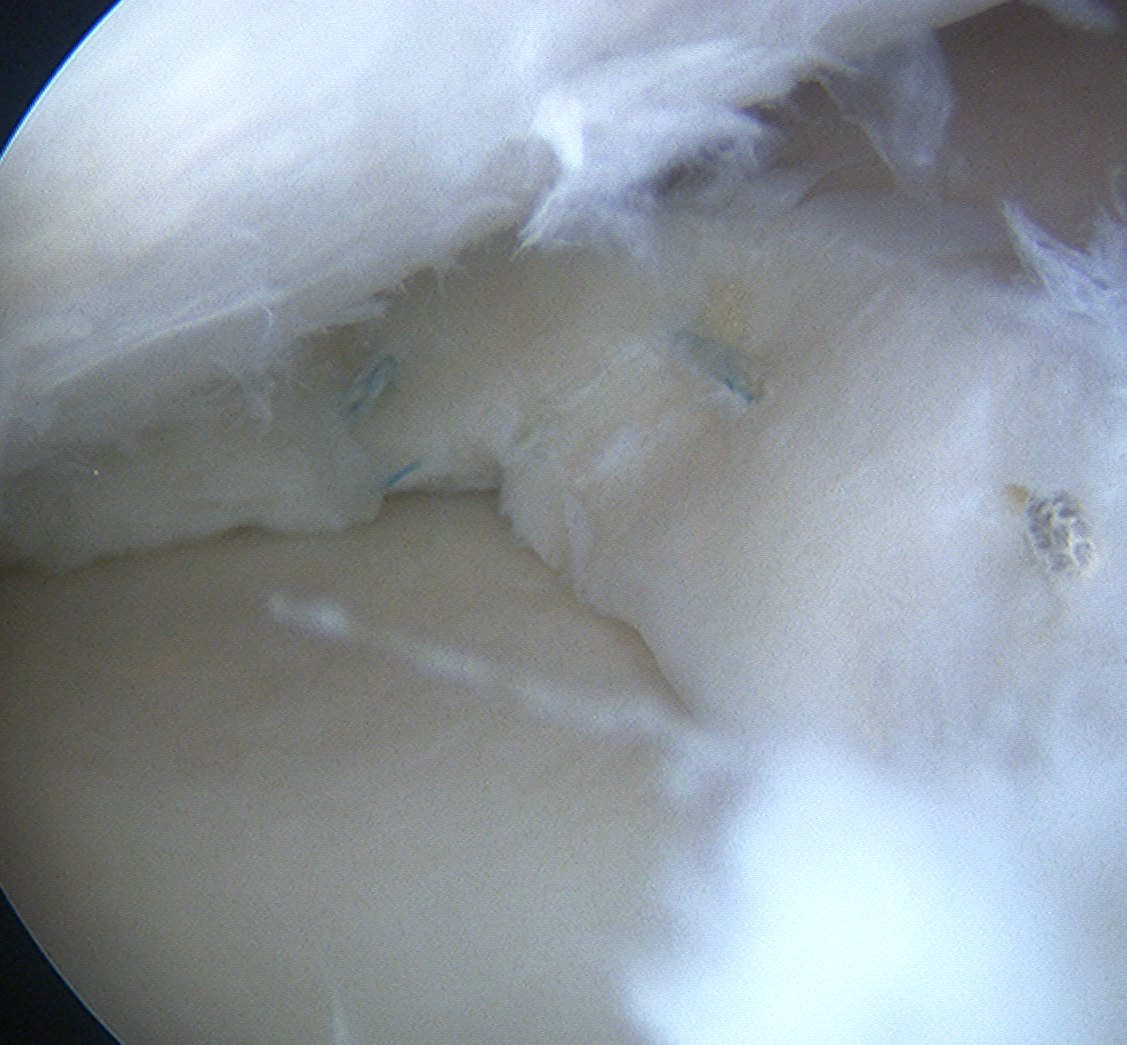
Pass the needles about the tear
- vertical or horizontal mattress sutures
- absorbable or non absorbable 2.0 suture
- every 2-3 mm
Tie sutures over capsule
- tie in extension or will break when patient extends leg

Posteromedial incision
- placed at the posterior aspect of MFC
- knee at 90°
- 3-4 cm long vertical incision
- behind MCL
- protect saphenous nerve which runs in fat above the sartorius
- open sartorius fascia, retract to protect nerve
- displace medial head gastrocneumius posteriorly
- expose capsule
Posterolateral incision
- centred on joint line, just posterior to LCL
- knee at 90o
- above biceps and therefore CPN
- palpate LCL anteriorly
- Biceps is retracted inferiorly to protect CPN
- must dissect lateral gastronemius off capsule and retract
- this protects CPN and posterior neurovascular bundle
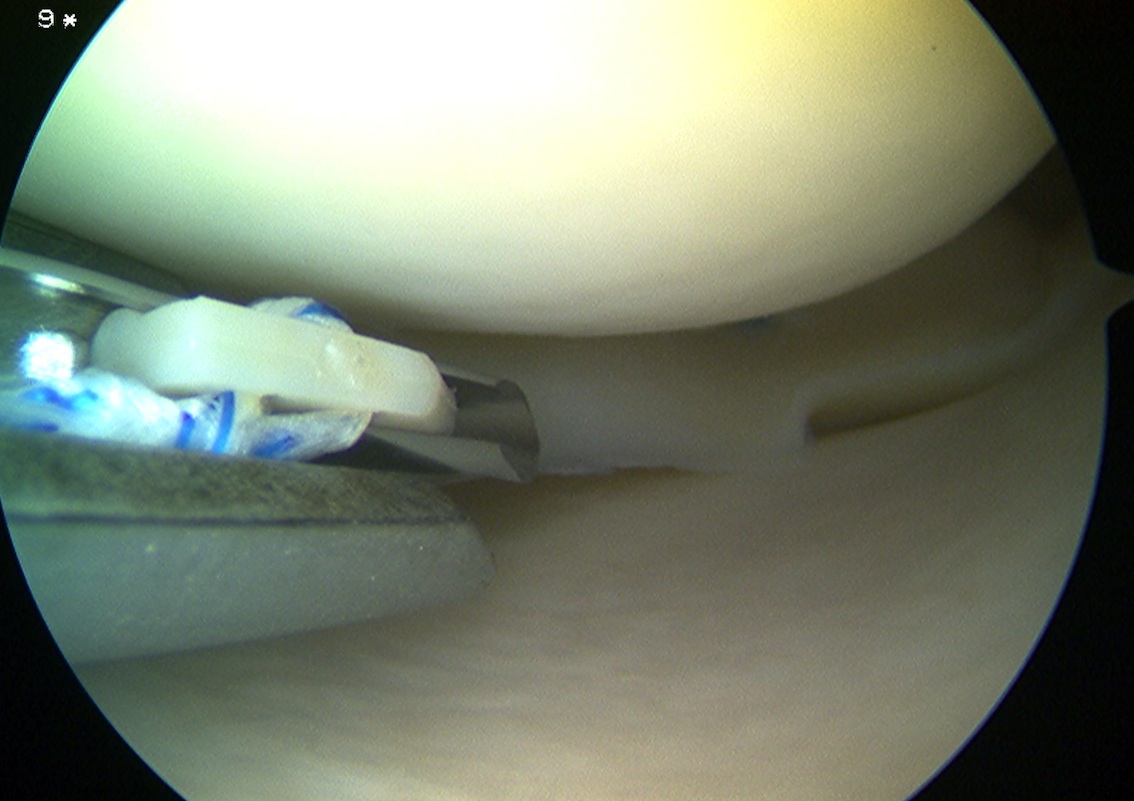
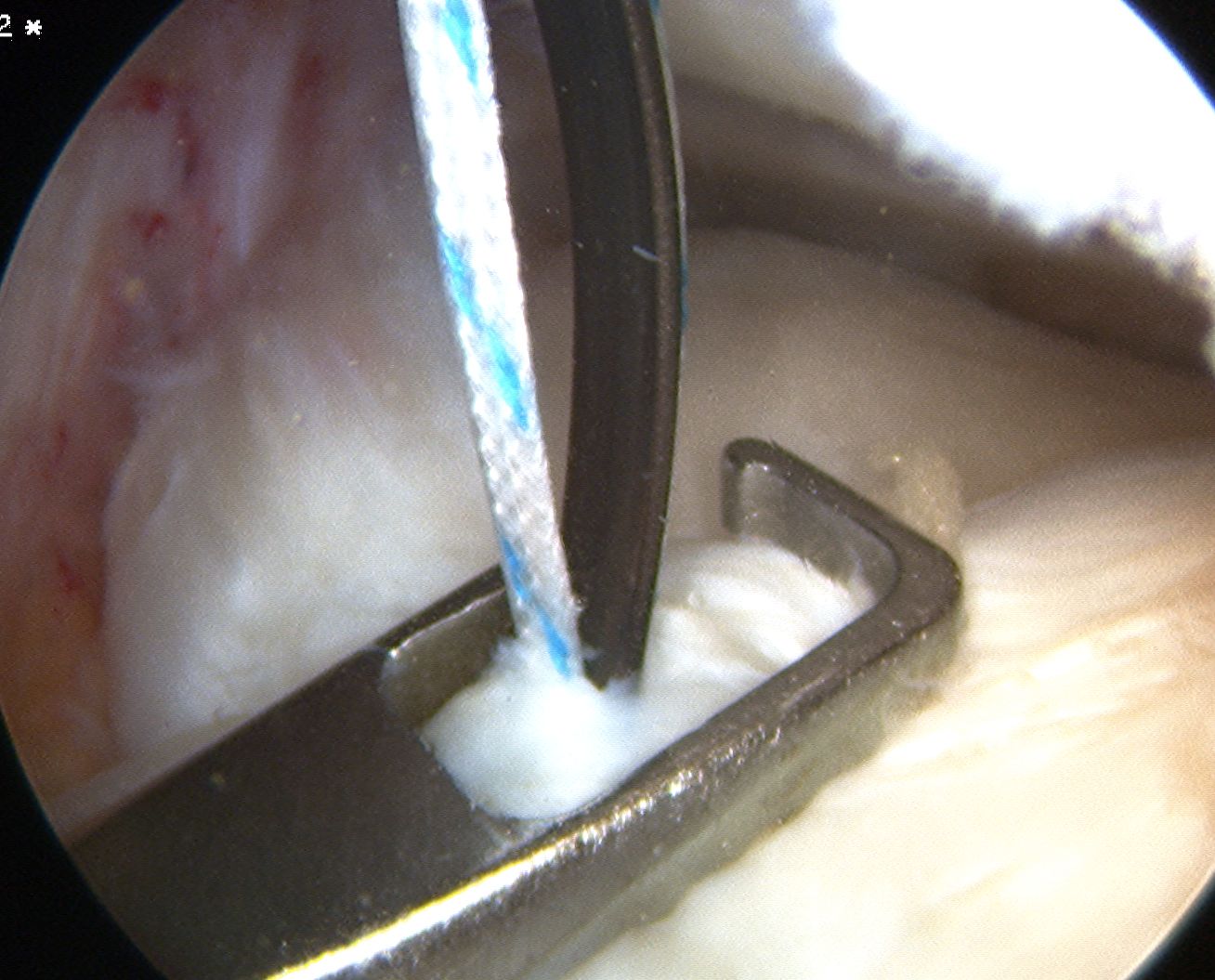
3. All inside
Instruments
- meniscal arrows (Biostinger, Meniscus Arrow)
- meniscal screws
- meniscal suture anchors (FasT-Fix, RapidLoc)
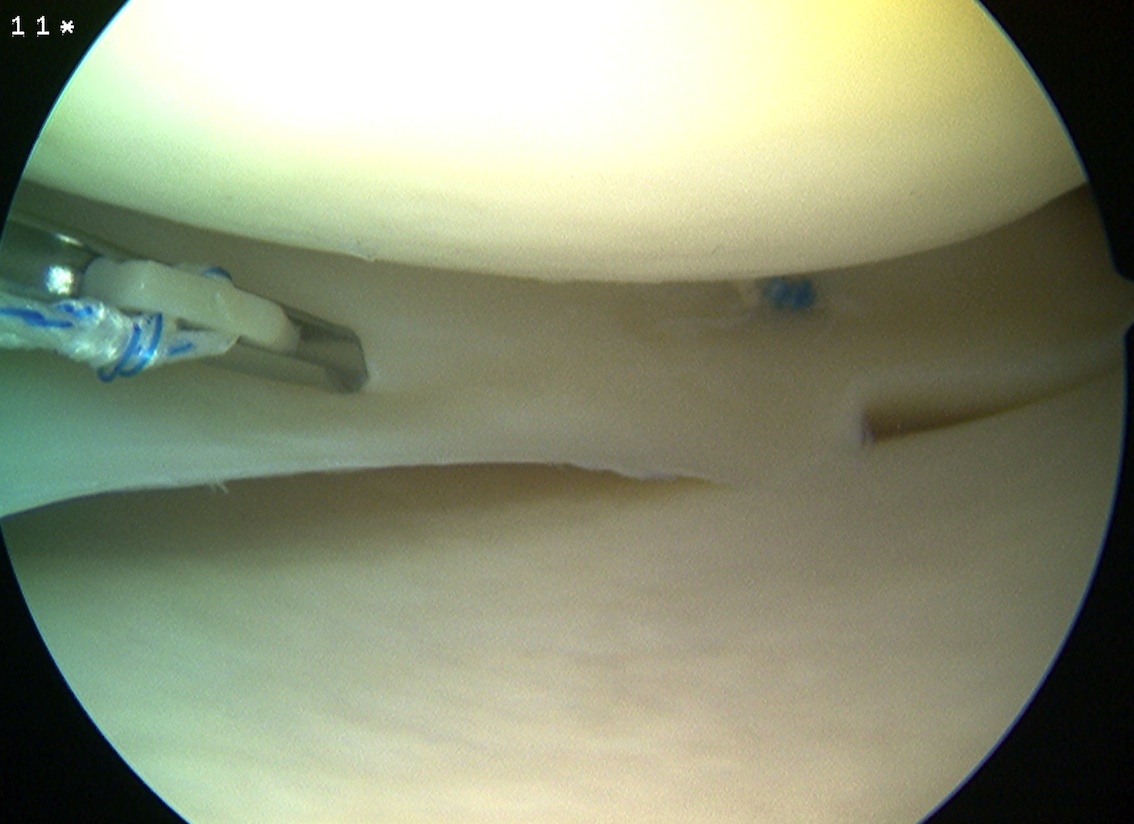
Technique FasT - Fix
- ipsilateral portal to view
- contralateral portal for instruments
- 2 x absorbable sutures anchors posteriorly
- may have to change portals for mensical body sutures
- pass first bioabsorbable anchors through meniscus and capsule
- retract and advance second anchor
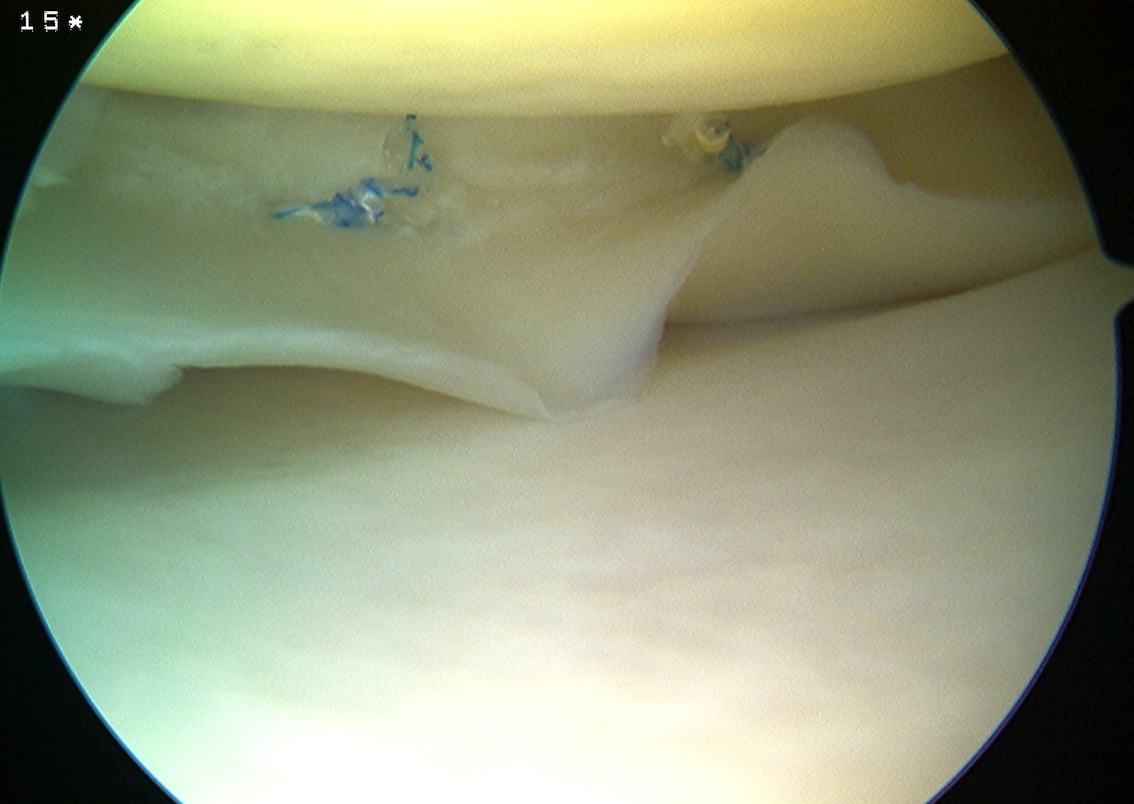
- place anchor through meniscus (horizontal) or into capsule alone (vertical)
- advance knot, cut

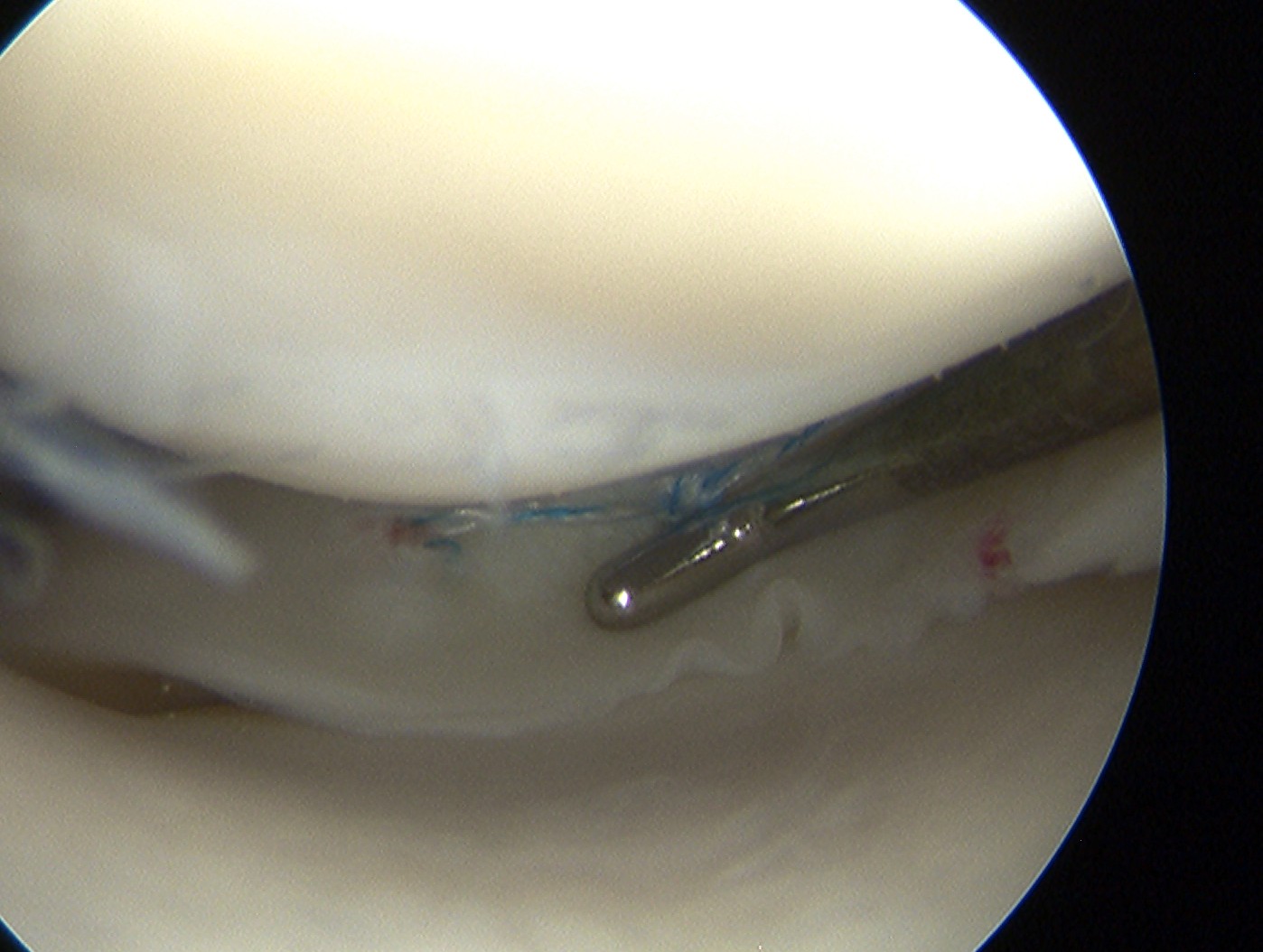
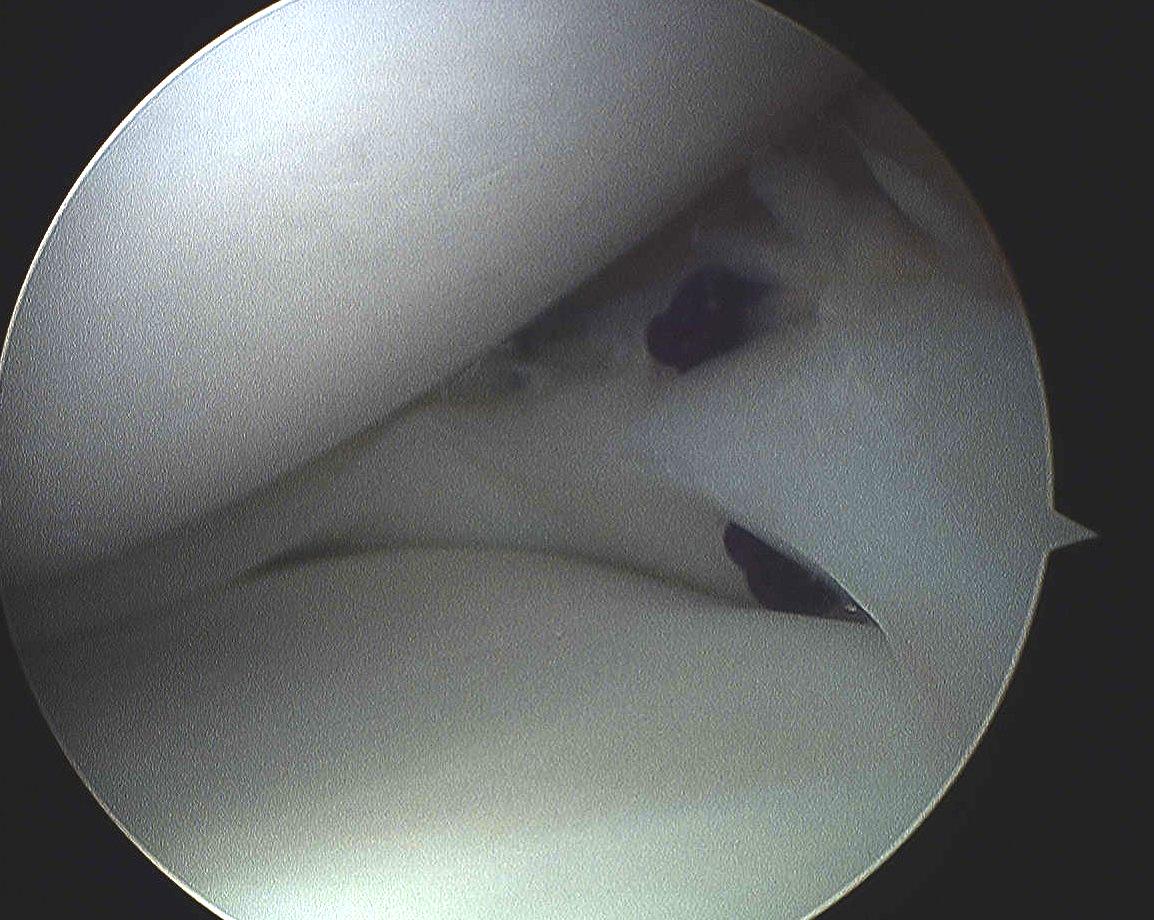
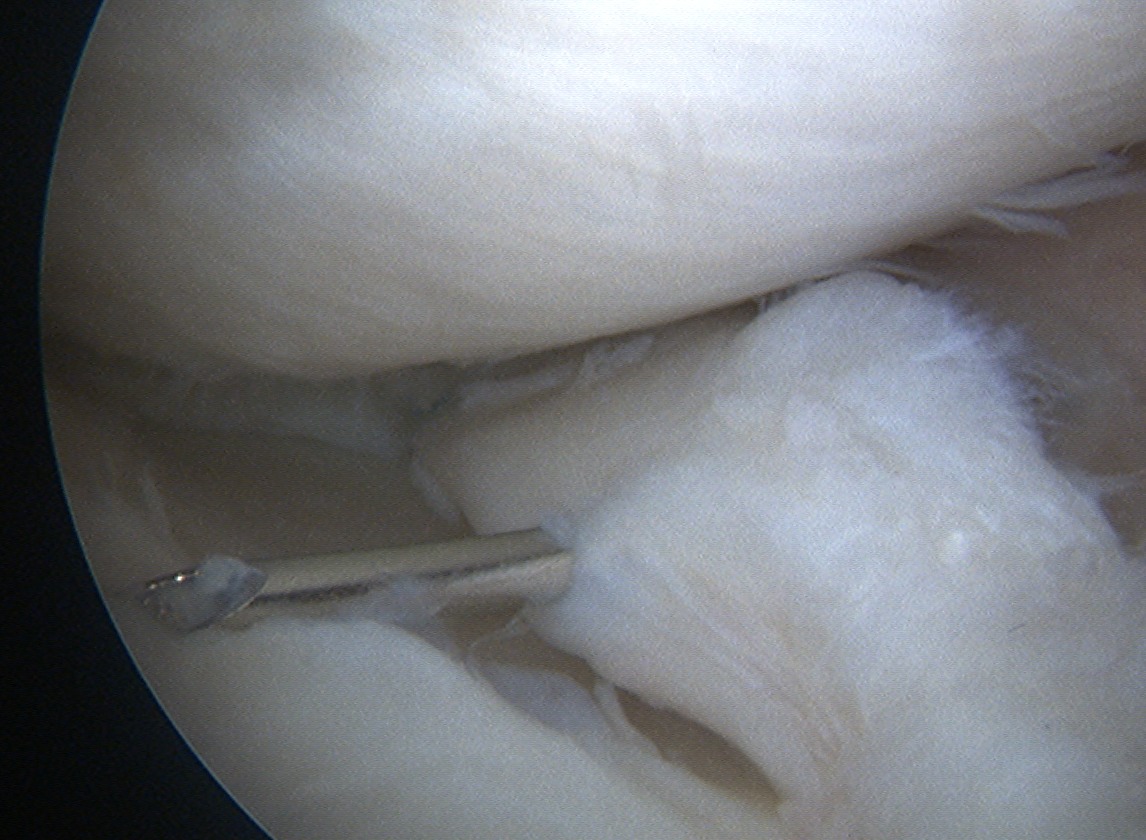
3. Outside in
Indicated for anterior horn tears
- very difficult to get angle on the tear
- either with all inside or inside out
A. Option 1
- camera in portal opposite to tear
- insert spinal needle through capsule and tear
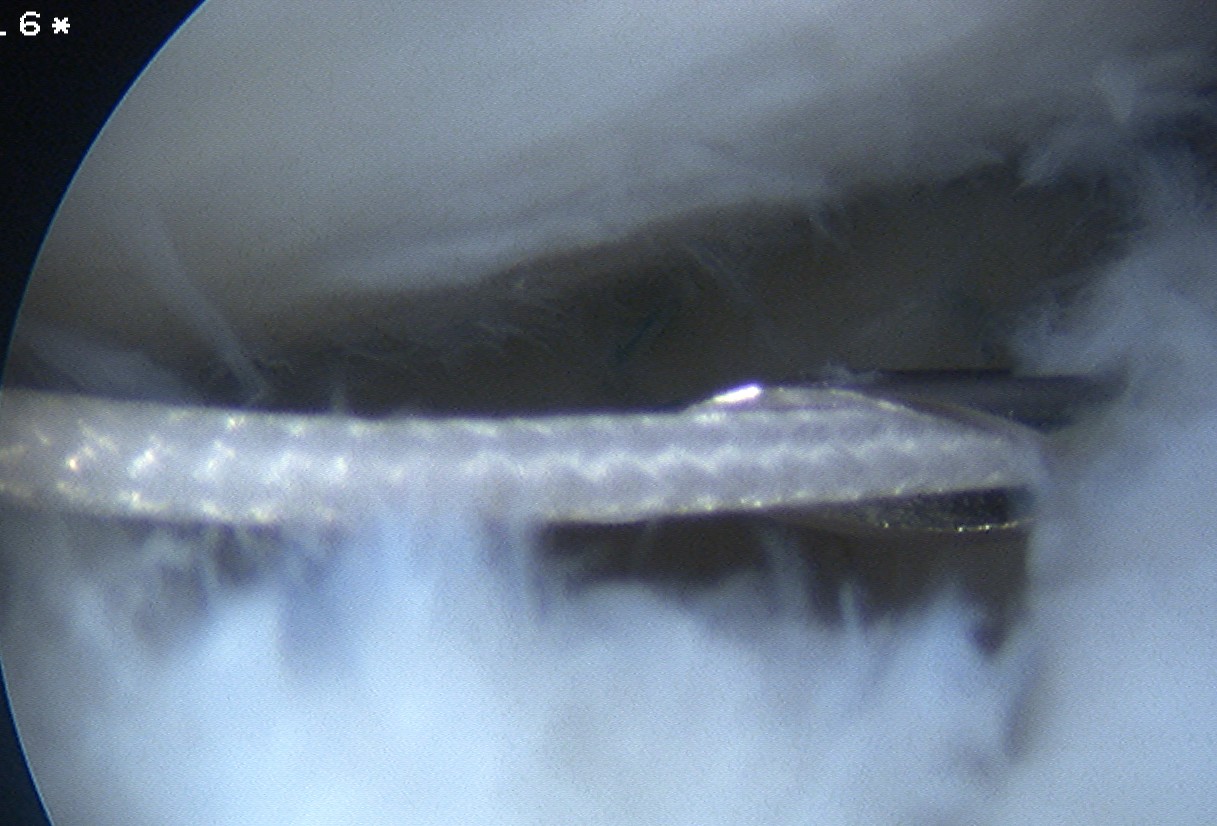
- insert 1 PDS via spinal needle
- retrieve suture via anterior portal, tie a knot in end
- secure meniscus with knot
- repeat above step
- tie 2 sutures over outside of capsule
B. Option 2
- insert PDS via spinal needle as above
- insert second spinal needle with loop PDS
- retrieve first PDS through that loop
- then pull single ended PDS back out through capsule
- tie over capsule
C. Company made sets
- insert 2 hollow bore needles through capsule and meniscus
- insert single ended suture through one needle separate needle
- insert wire loop through other needle and retrieve
- tie over capsule through separate skin incision


D. Anchor repair
- insert anterior suture anchor
- pass sutures through meniscus and tie down
- technique used in meniscal transplant

Ramp lesion
4. Meniscal Root Repair
Definition
- tear of insertion of posterior horn of meniscus
- difficult to fix
- must repair down to bone
Technique
- ACL guide
- drill hole up into mensical root insertion
- use suture passer to secure meniscal root
- retrieve sutures down through bone tunnel in tibia
- tie over screw post


Post operative rehab
Avoid weight bearing in flexion > 90o
- weight bear in extension / splint for 6 weeks
- range to 90o NWB