knee
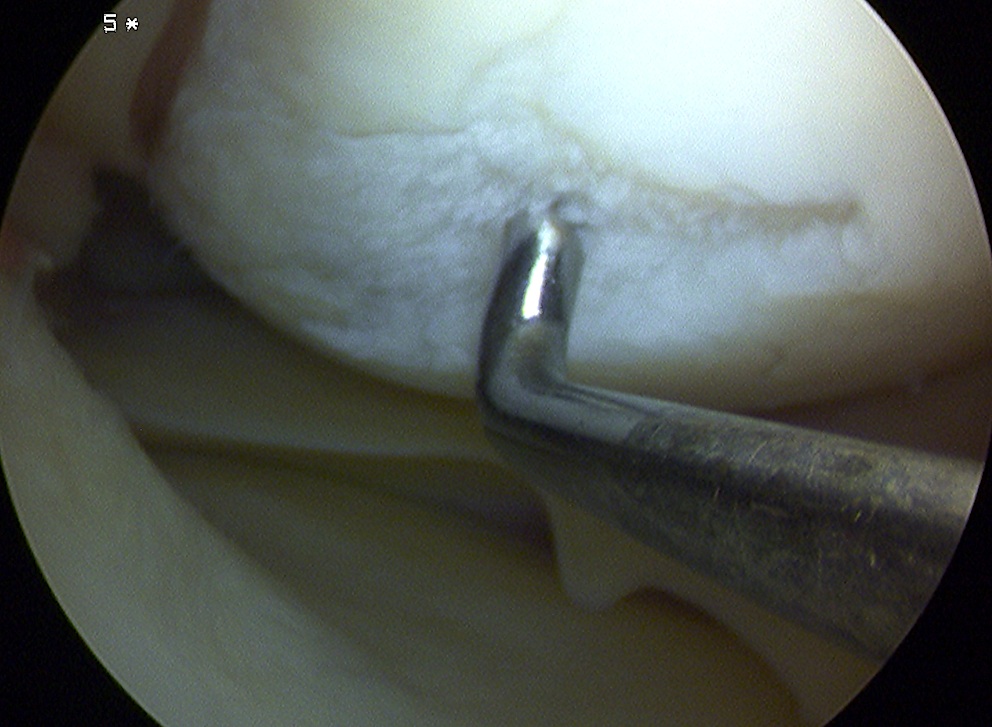
Fat Pad Syndrome
Definition
Hoffa's syndrome
- impingement of the fat pad with knee ROM
Epidemiology
Rare
Diagnosis of exclusion
Theory
May be more prevalent in patients with intact ligamentum mucosum
Diagnosis
Hoffa's sign
- apply pressure to fat pad each side of patella tendon with knee in flexion
- extend knee
Knee
Approaches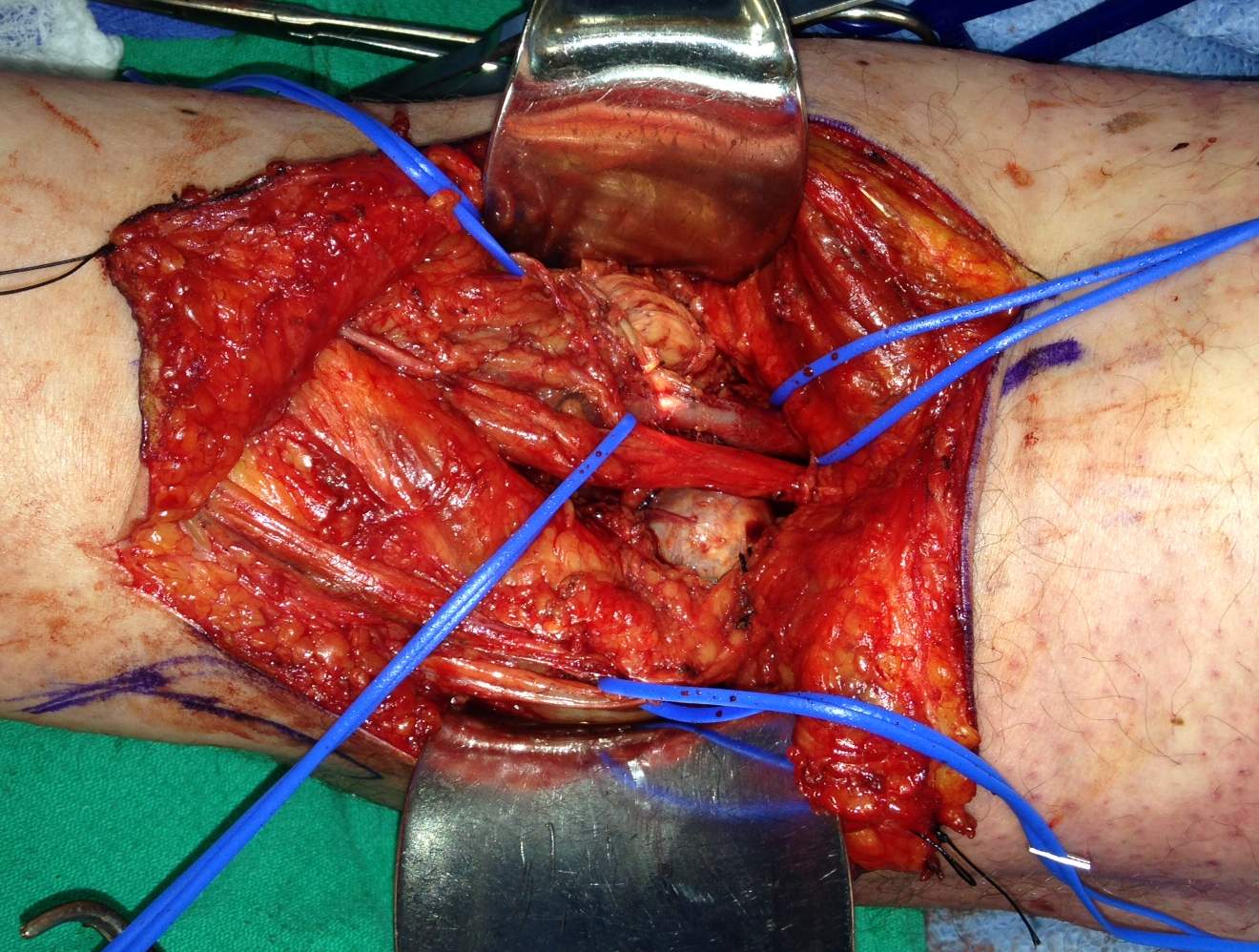
Medial Parapatellar
Medial
Lateral
Posterior
Modified Posterior
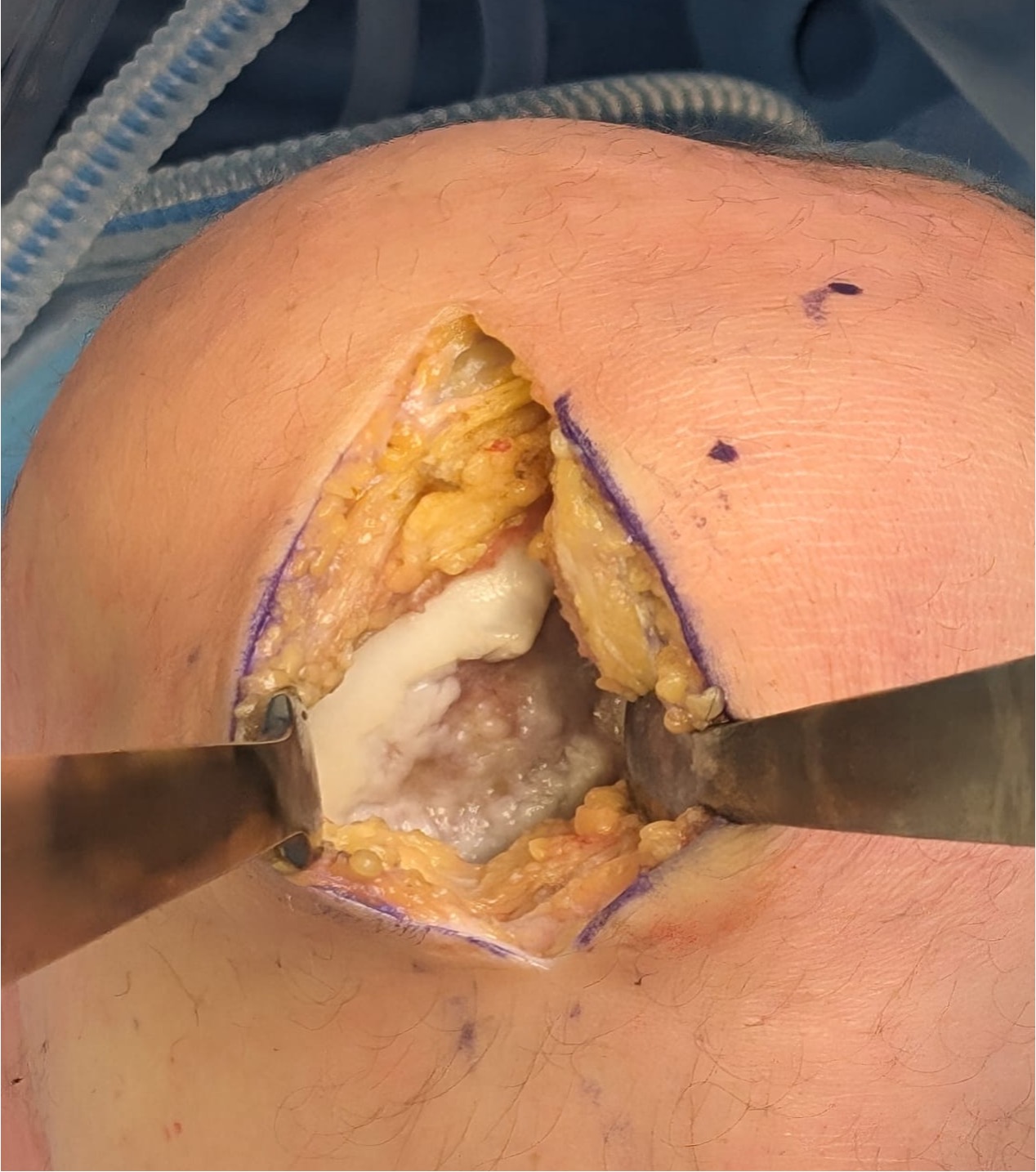
Medial Parapatellar Approach
Indications
Synovectomy
Patellectomy
TKR
Technique
Meniscal Repair
Indications for Repair
Only 20% repairable
1. Red / Red longitudinal tear
- outer 3mm / meniscocapsular junction

PVNS
Definition
Pigmented Villo-Nodular Synovitis
- benign inflammatory process that arises in synovial tissues
- contains significant amounts of hemosiderin
Epidemiology
Age: 20 - 50
Sex: M > F
Types
A. Diffuse
- throughout joint synovium
- more difficult to treat / excise fully
Synovial Chondromatosis
Definition
Chondroid Metaplasia of synovium affecting large joints
Nodules of hyaline cartilage
- formed in the subsynovial layer of joint capsules
Epidemiology
Rare lesion
Most common in 20's and 30's
Sex: M > F (2:1)
Monoarticular
Site
Mass Behind Knee
DDx
Baker's Cyst
Popliteal Anerysm
Soft tissue sarcoma
Osteosarcoma / Parosteal OS
Hemangioma / AVM
Note:
Always do xray for calcification
A Bakers cyst / aneurysm can be calcified
Loose Bodies

Source
OCD
OA - Osteophytes
Meniscus
Symptoms
Pain
Locking
Clicking
Can cause chondral damage
Xray
OA Loose Bodies
Patellar tendonitis
Definition
Patellar Tendinitis
Epidemiology
Most common in athletes
- especially if involved in running, jumping and kicking
- over use injury
Basketball players
Aetiology
Chronic overload v inferior patella impingement
Schmidt et al Am J Sports Med
- dynamic MRI in patients with jumper's knee v controls
- no evidence of impingemnt
Knee & Foot
Principles
Foot
A little equinus is better than calcaneus
A little valgus is better than varus
A little varus is better than severe valgus
TA lengthening is most over used operation in CP
Knee
A little knee flexion is better than recurvatum
Knees
Problems
Tight hamstrings