Indications
Young patient
- previous total or near total meniscectomy
- developing joint line pain
- early chondral changes
- normal anatomic alignment
- stable or reconstructable knee
Contra-indications
> Grade 2 Chondral changes
Farr et al Am J Sports Med 2007
- combined mensical transplantation with ACI
- improved patient outcomes
Aim
To prevent progressive cartilage damage
Issues
1. Graft selection
- usually fresh frozen
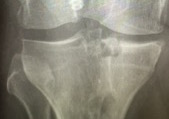
2. Graft sizing
Size needs to vary < 5% compared with original
Options
- X-rays accurate in 79% cases
- CT scan
- MRI accurate to within 5 mm
3. Surgical technique
Secure fixation important
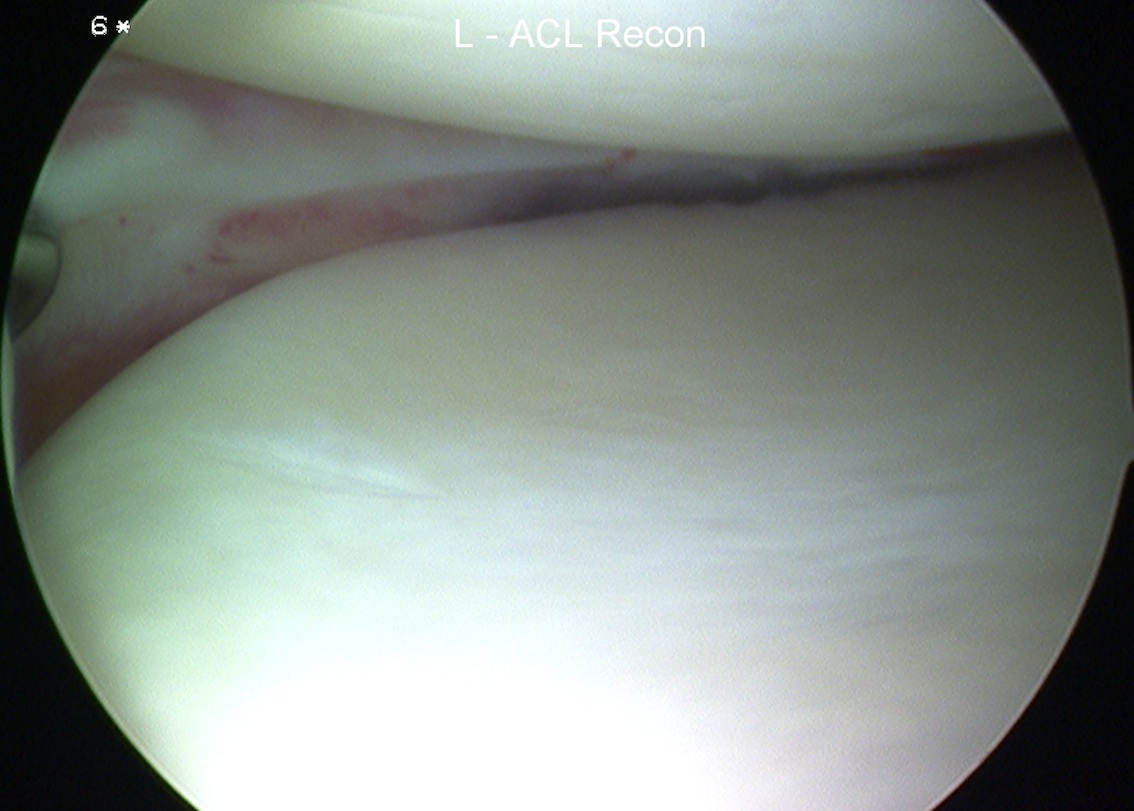
Technique
Bone in slot techique
- maintain meniscal attachment
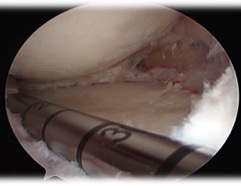
- prepare bone graft to fit in 8 mm slot
Small medial or lateral parapatella to make trough
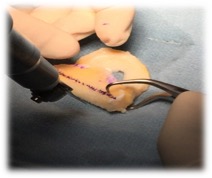
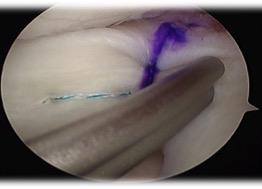
- prepare meniscus
- leave margin of meniscus to allow suture to
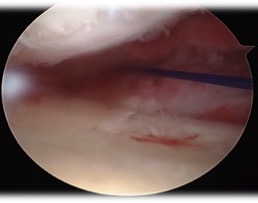
- mark site with needle
- just on inner margin of articular surface
- mark with shaver
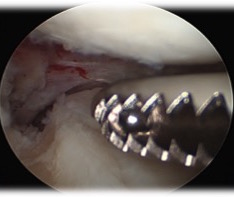
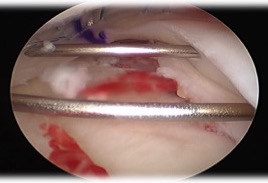
- insert guide pin, drill over, then insert box cutter
- carefully clean out with shaver



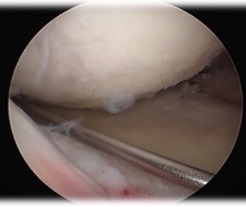

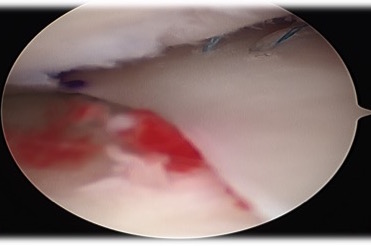
Pass graft
- place suture at junction of body and posterior horn
- make posteromedial approach
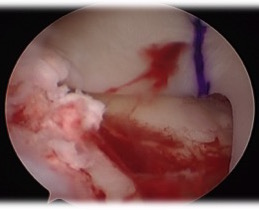
- insert graft bone into slot
- secure with screw
- flip meniscus
- secure posterior horn with all inside sutures, body with inside out, anterior horn with outside in
Results
McCormick et al Am J Sports Med 2014
- 172 patiens, mean age 30 +/- 10 years
- 95% survival at 5 years
- 22% arthroscopic debridement
- 4.7% need revision transplant or TKR