



Epidemiology
Metatarsal fractures
- 5 - 6% of all fractures
- 70% of these involve 5th metatarsal
Types
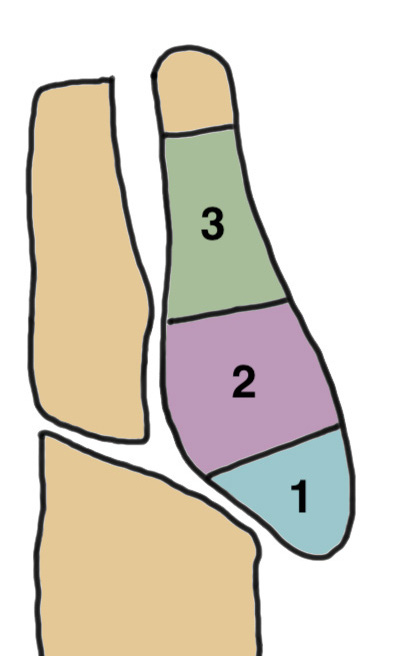
Base of 5th - Zone 1 / 2 / 3
Metatarsal shaft - spiral fracture
Metatarsal neck fractures



Base Shaft Neck
Base of 5th metatarsal fractures
Classification
| Zone 1 | Zone 2 | Zone 3 |
|---|---|---|
|
Tuberosity avulsion fractures
|
Metaphyseal-diaphyseal junction Involves the 4th / 5th MT articulation |
Distal to the 4th / 5th MT articulation Proximal diaphysis |
| Inversion injuries |
Jones fracture Acute adduction injury |
Repetitive stress fracture Athletes |
 |
 |
|
| Incidence: 93% | 4% | 3% |
Dean et al Foot Ankle Spec 2012
- systematic review
- in the literature there is poor differentiation between Zone 2 and Zone 3
Zone 1 Metatarsal fracture
Definition
Tuberosity avulsion fracture
- extra-articular
- may extend into cuboid-metatarsal joint
Etiology
Peroneus brevis contracture following inversion
Xray


Differential diagnosis
| Apophysis | Os peroneum | Os Vesalianum |
|---|---|---|
|
Longitudinal Does not enter cuboid-MT joint
Iselin's disease / Traction apophysiits |
Accessory bone - well rounded shape
Within peroneus longus tendon |
Accessory bone - well rounded shape
Within peroneus brevis |
|
Appears - female 9 - 11 - male 11 - 14 Fuses 3 years later |
Lateral aspect of the cuboid Common - in up to 25% of feet |
Very uncommon Usually asymptomatic
|
 |
 |
 |
| BMJ case report | www.boneschool.com/os-peroneum | Literature review |
Nonoperative management
- systematic review of 627 zone 1 fractures
- union rate nonoperative: 93%
- union rate operative: 95%
Valkier et al J Foot Ankle Surg 2020
- 20 avulsion fractures treated with surgery
- 30 treated nonoperative
- nonoperative: 36% asymptomatic nonunion
- no functional difference between two groups at 1 year
- RCT of 46 displaced Type 1 avulsion fractures
- better function at 6 months, earlier return to work
- no difference at 12 months
Operative management
Indications
- intra-articular and > 30% cuboid joint
- displaced > 2 mm
Options
- IM screw
- hook plate
- suture anchor




Arthrex hook plate technique video
Zone 2 / 3 Metatarsal Fracture
Definition
Zone 2 Jones fracture
- transverse fracture of 5th metatarsal shaft
- 1.5cm from base
- diaphysis / metaphysis junction
- extends into 4th / 5th metatarsal joint
Zone 3 Metatarsal fracture
- diaphyseal stress fracture
- distal to 4th / 5th metatarsal joint
- secondary to repetitive distraction force
Nonunion
Blood supply
Watershed area in the proximal metaphysis
Correlates to area of poor healing
Nonunion rates
- systematic review of 600 zone 2 / Jones fractures
- union rate nonoperative: 77%
- union rate operative: 96%
- refracture rate 2% in both groups
- systematic review of 400 5th metatarsal stress fractures
- operative union rate: nonunion 4%, refracture 7%
- nonoperative: nonunion 33%, refracture 12%
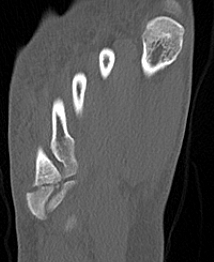
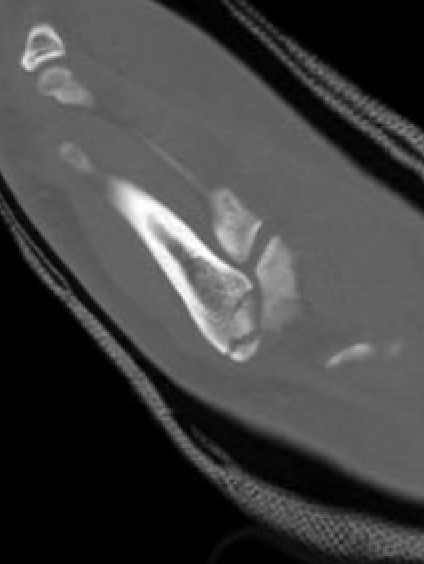
Xray
Zone 2 fractures


Union of zone 2 fracture with nonoperative care



Progression to nonunion of zone 2 fracture with nonoperative care


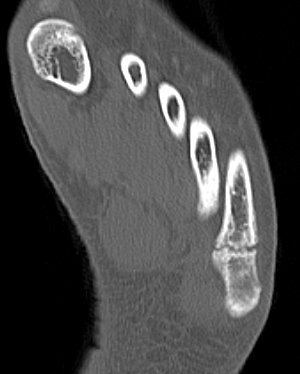
Progression to nonunion of zone 2 fracture with nonoperative care



Progression to nonunion of zone 2 fracture with nonoperative care
Zone 3 Fractures

Progression to nonunion of zone 3 fracture with nonoperative care
Torg Classification
| Type I | Type II | Type III |
|---|---|---|
| Acute | Delayed union | Nonunion |
|
Narrow fracture line No sclerosis No cortical reaction No periosteal hypertrophy |
Increased fracture line Both cortices Some sclerosis Some periosteal hypertrophy |
Significant sclerosis Significant cortical hypertrophy |
 |
 |
 |
Nonoperative management
Kadiyala et al J Orthop Trauma 2024
- 475 Zone 2 fractures treated nonoperative
- 2/3 non weight bearing
- 1/3 weight bearing
- nonunion rate 6% at 10+/-8 weeks
Operative management
Indications
- displaced fractures > 2 mm
- nonunion
- athlete

Displaced fracture Nonunion
Options
Intramedullary screw
Plate fixation
- systematic review of 10 studies and 300 patients
- screw versus plate
- no difference in outcomes or complications
Intramedullary Screw


Screw fixation Zone 2 nonunion


Screw fixation Zone 2 nonunion

Screw fixation Zone 2 nonunion


Screw fixation Zone 3 nonunion
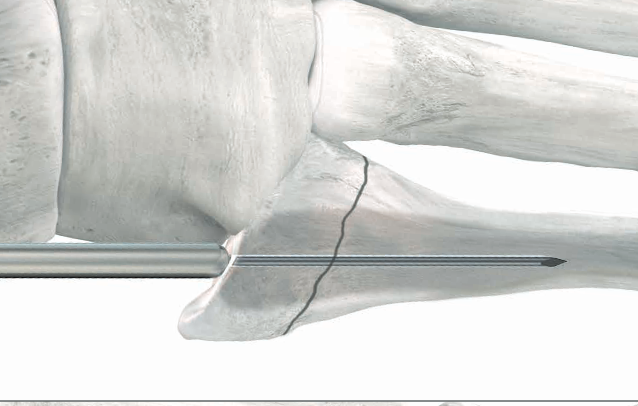
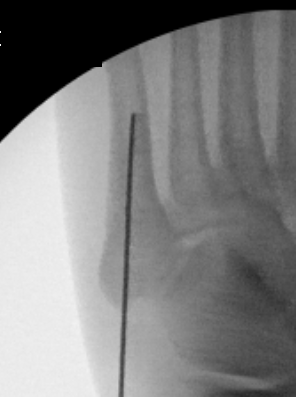
Technique



Paragon IM screw technique PDF
Entry point
- 5th metatarsal is not straight
- high and medial to get straight shot
- avoids plantar insertion peroneus brevis
- screw diameter 3.5 / 4.5 / 5.5 / 6.5
- screw threads must be distal to fracture site to allow compression
Arthrex technique IM screw 5th metatarsal video
Vumedi IM screw 5th metatarsal video
AO foundation surgical technique



Biological augmentation
Biologics
- autograft
- bone marrow aspirate
- systematic review ORIF +/- biological augmentation
- ORIF + biologics: union 98%
- ORIF alone: union 94%
5th Metatarsal Shaft Fractures
Definition
Spiral fracture of the shaft of the 5th metatarsal
Dancer's fracture
Gonzalez et al Foot Ankle Spec 2024
- 37 spiral 5th metatarsal fractures
- 78% women, average age 50

Nonoperative management
Gonzalez et al Foot Ankle Spec 2024
- 37 spiral 5th metatarsal fractures
- treated weight bear as tolerated
- all healed by 3 months
- 27% mild pain
- 3% significant pain
- 33 shaft fractures treated nonoperatively
- faster return to function with shoe versus boot
Operative management
- systematic review of management spiral 5th metatarsal fractures in athletes
- union rate nonoperative and operative 99%
- return to sport: nonoperative 15 weeks, operative 22 weeks

