Indications
Irreducible fractures
- fractures that cannot be reduced except by operation
Unstable fractures
- fractures that are inherently unstable and prone to re-displacement after reduction
Fractures that unite poorly
- i.e. fractures of the femoral neck
Pathological fractures
- fractures in which bone disease may prevent healing
Multiple fractures
- where fixation of one fracture facilitates treatment of the others
Fractures in patients who present nursing difficulties
- i.e. paraplegics, multiply injured patients, elderly
Principles of Internal Fixation
Aim
- produce stable fracture fixation
- minimum of devascularisation
- early motion and partial loading
Stable fixation
- fixation that prevents motion of the fragments
- stable fixation is best represented by a simple fracture with a rigid plate applied across the fracture in compression
- the introduction of compression introduced stability
- stable fixation restores the load bearing capacity
Compression
- produces preloading, maintaining close contact of the fragment surfaces
- produces friction which resists transverse displacement and torque about the long axis
- allows the transfer of force from fragment to fragment rather than via the implant
Strain
- relative deformation of a tissue
- displacement of fragments divided by the width of the fracture gap
- represents the degree of instability
- at very low levels of strain the bone heals by primary healing
- at intermediate levels healing is by callus
- at high levels non-union occurs
Instability is best tolerated by multi-fragmentary fractures
- the displacement is distributed over several interfaces
- the individual strain is low
Strain is very high for bone fragments separated by a single narrow gap
- these fractures are very intolerant of even minute displacement
Types of Internal Fixation
1. Lag screws
2. Plates
3. Intramedullary Nails
4. Tension Band Wiring
Lag Screws
Stability is achieved by compression and bone contact
- load transfer occurs directly from fragment to fragment and not via the implant
- should be placed perpendicular to the fracture line
- can apply 2000-4000N
- 1 screw is never strong enough to achieve stable fixation and 2 or 3 screws are required
- provide excellent stability but their strength is usually inadequate to resist displacement under functional loads
- are therefore usually combined with a neutralisation plate


Plates
1. Neutralisation plate
2. Buttress plate
3. Tension Band plate
4. Bridging Plate
Neutralisation plate
- used to protect lag screws
- conduct part or all of the force from one fragment to another
- protect the fracture fixation from bending, shear, and rotation
- e.g. lateral malleolus fractures - lag then apply a derotation plate


Buttress plate / Antiglide Plate
- physically protect underlying thin cortex
- often used with metaphyseal fixation
- buttress is intra-articular (tibial plateau)
- antiglide is metaphyseal - diaphyseal



Compression plate (DCP - dynamic compression Plate)
- compression generated either by a tension device or by the dynamics of the plate itself (DCP)
- plate should be applied to the tension side of eccentrically loaded long bones
- produces fracture compression and resists tension forces
- DCP plate can produce about 600N (lag screw 2000-4000N)
- underlying bone loss due to interruption of blood supply / periosteum injury
- limited by decreasing the surface contact of the plate i.e. LCDCP (limited contact DCP)
- plate should be over bent to produce compression of the far as well as near cortex
- inner screws should be applied first


Bridging Plate
- used in the treatment of some multifragmentary fractures i.e. femur
- instead of individually fixing each fragment
- minimal disruption to blood supply
- reduction is performed indirectly
- compression is only sometimes possible
Concept
- 6 holes over each fragment if possible
- only fill 50% in intermediate fragments
- i.e. 3 bicortical screws sufficient
- near far near far concept
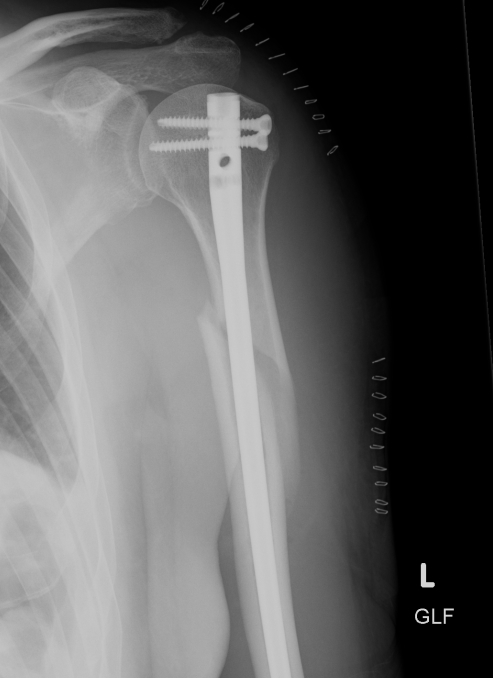
Intramedullary Nails
Indication
- for fixation of the diaphysis of long bones
- reamed vs unreamed
- initial nails relied on interference fit on either side of the fracture and hence could only be successfully applied to midshaft fractures
- interlocked nails have expanded indications to distal and proximal 1/3 shaft fractures


Tension Band Wiring
Concept
- relies upon compression by the dynamic component of the functional load
- allows some load induced movement
- really only suitable for metaphyseal regions
- eg. patella and olecranon

Screws
Cortical screws
- greatest SA of thread for any given length
Cancellous screw
- smaller core diameter
- larger thread diameter
- threads further apart (increased pitch)
Splints
Plaster
Roll of Muslin stiffened by dextrose or starch
- impregnated with hemihydrate of calcium sulfate i.e. dehydrated gypsum
- when H20 is added, the calcium sulfate takes up its water of crystallization
- exothermic
Fiberglass
- knitted fiberglass
- 45% polyurethane resin
- 55% fiberglass
- prepolymer is methylene bisphenyl di-isocyanate (MDI), which converts to a nontoxic polymeric urea substance
- MDI molecules have isocyanate end-groups that react with any molecule containing an active hydrogen
- exothermic reaction