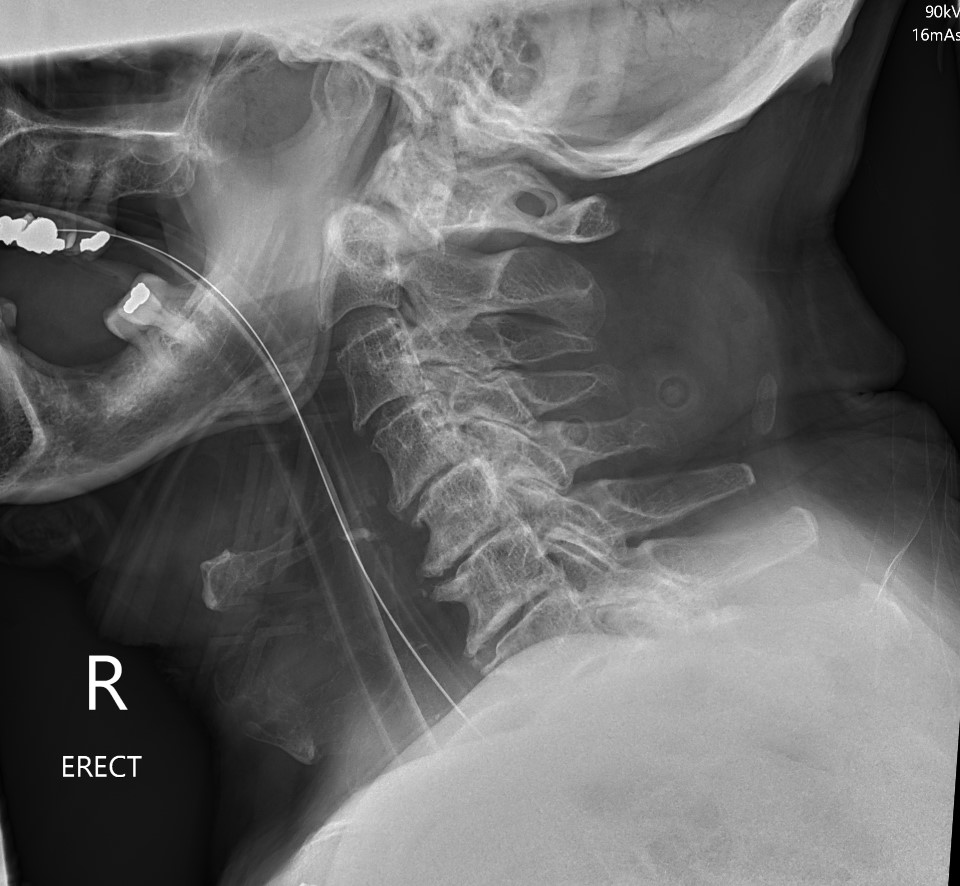

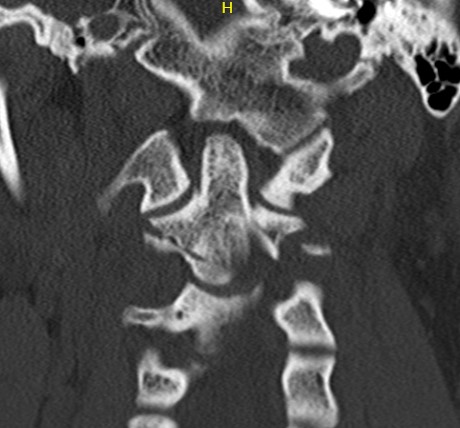
Anatomy
Superior projecting bony element of C2 / axis
C1 / atlas rotates around the dens to provide cervical rotation
Etiology / Epidemiology
Young - high energy injury
Elderly - low energy injury
Typically hyperextension injury
20% of all cervical spine injuries
Most common cervical fracture in the elderly
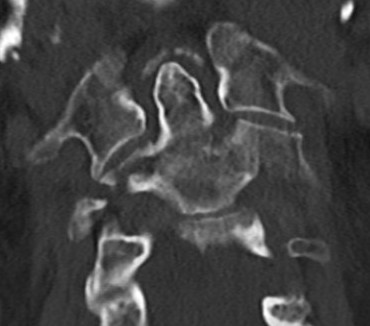
Classification Anderson & D'alonzo
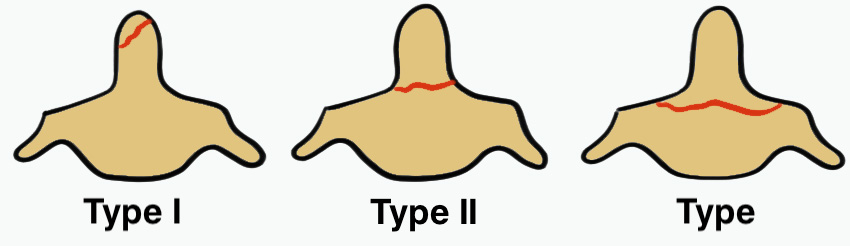
Type 1
Tip avulsion
- alar ligament avulsion
- fracture off one side of tip of odontoid process
- rare
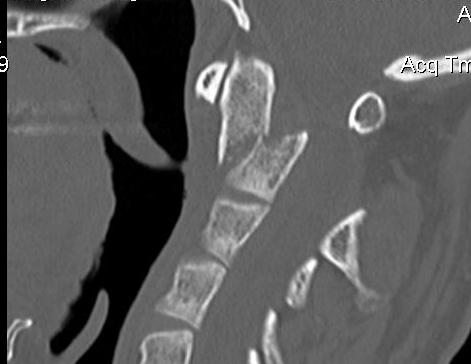
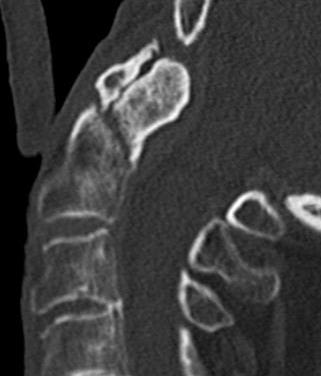
Type 2
Fracture of base of odontoid process
- most common type
- > 50%

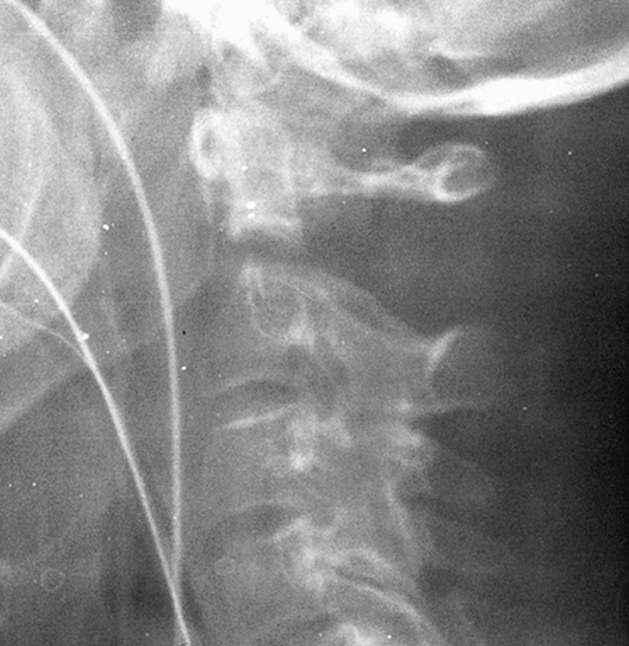
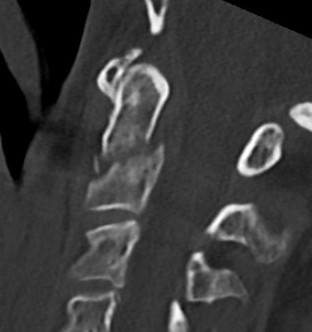
Type 3
Fracture through body of axis

Symptoms
Neurological injury rare due to large cross sectional area of spinal canal
Dysphagia due to retropharyngeal hematoma
Myelopathy symptoms
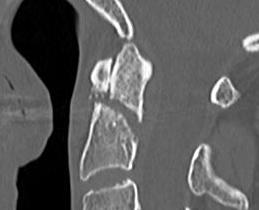
Type I Dens Fracture
Typically stable
Perform flexion / extension views
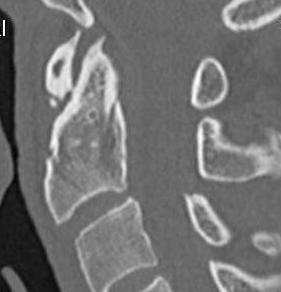
Type II Dens Fracture
Issue
Stability
Union
Elderly
Non-union
Vascular watershed area
- at base of odontoid
- increases risk of nonunion
Risk factors for nonunion
- 69 patients with acute type II fractures treated with halo vest
- union 32/69 (46%)
- nonunion associated with:
- fracture gap > 1 mm
- posterior displacement > 5 mm
- delay in treatment > 4 days
Management Type II
Grauer classification of Type II
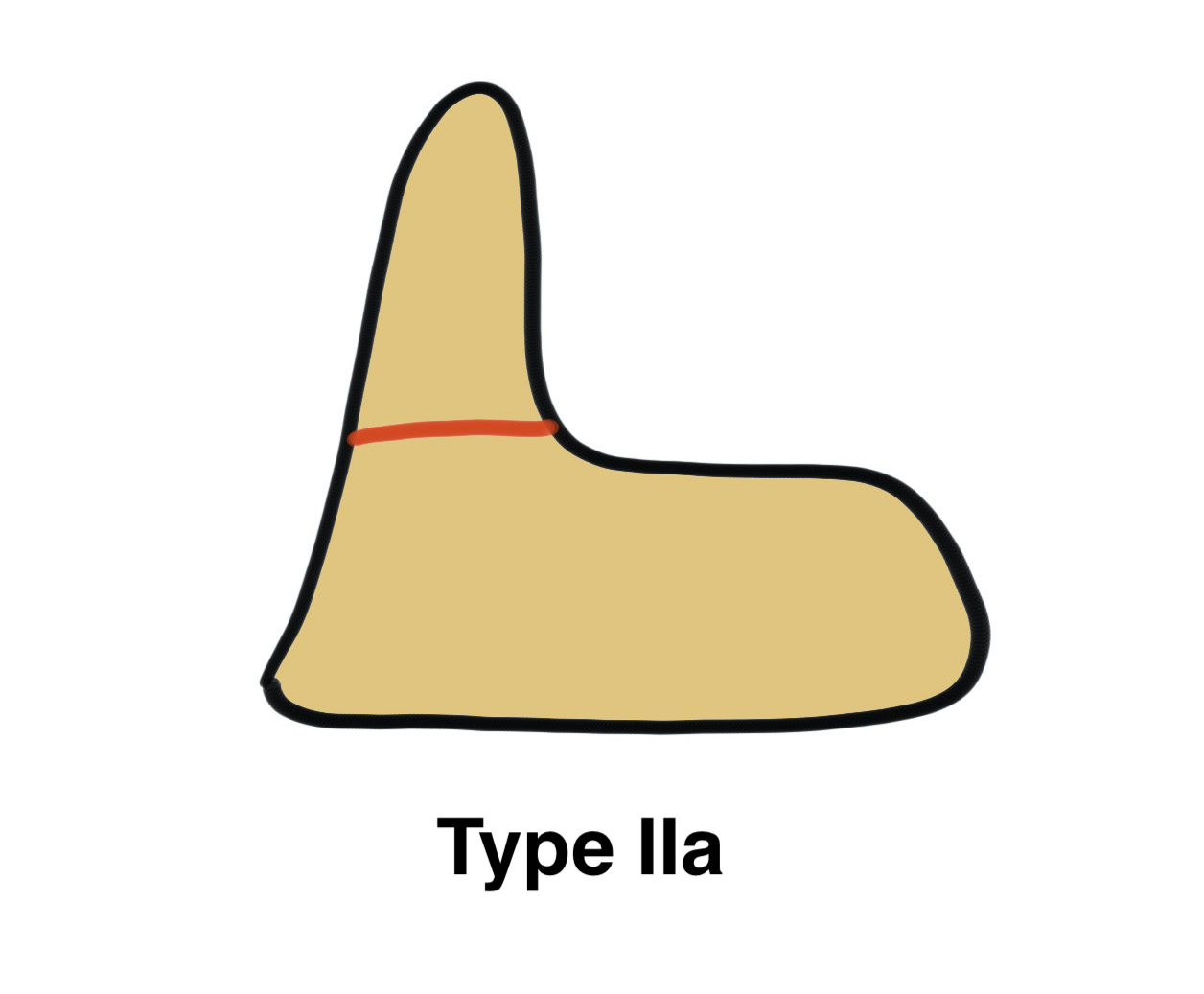
| Type | Definition | Management |
| Type IIa |
Non or mimimally displaced No comminution |
Non operative treatment |
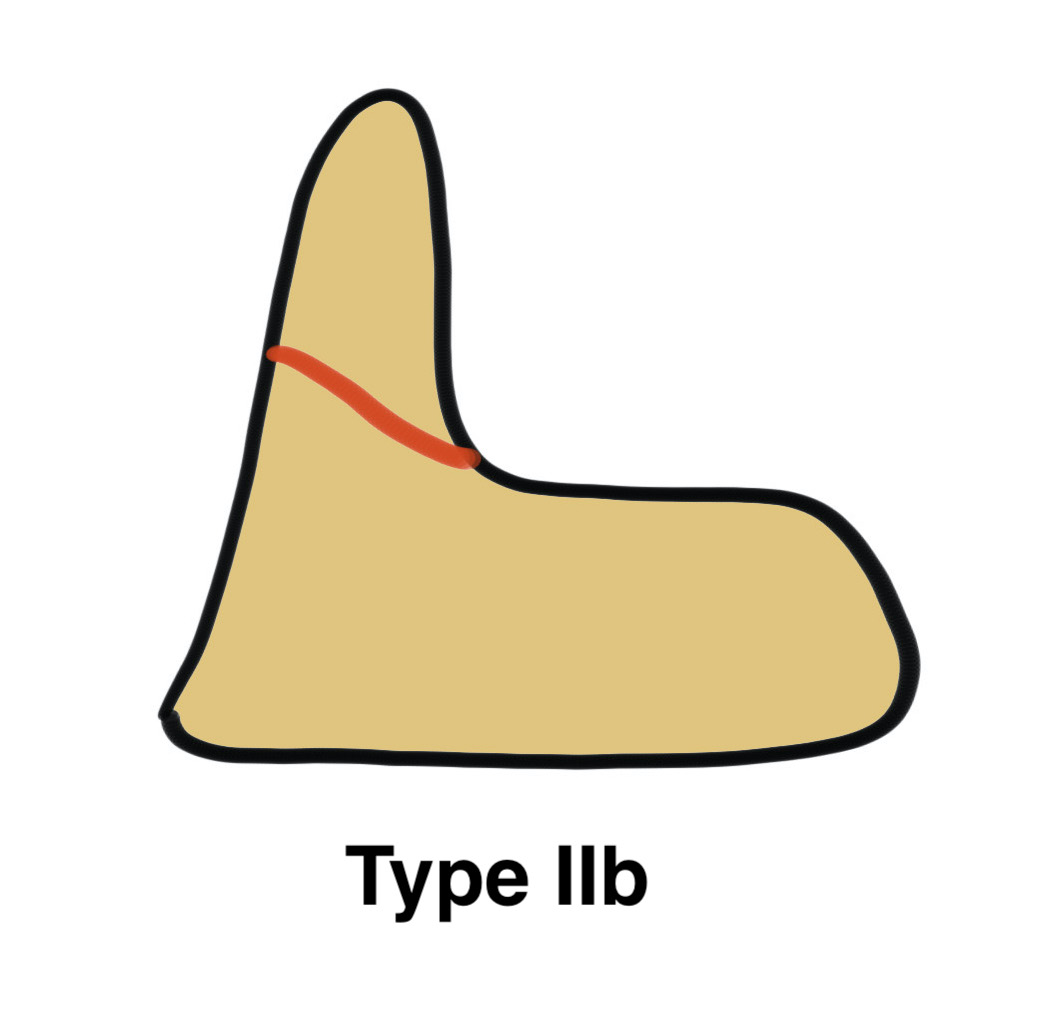
| Type IIb |
Displaced Fracture line anteror-superior to postero-inferior |
Potentially suitable for anterior odontoid screw |
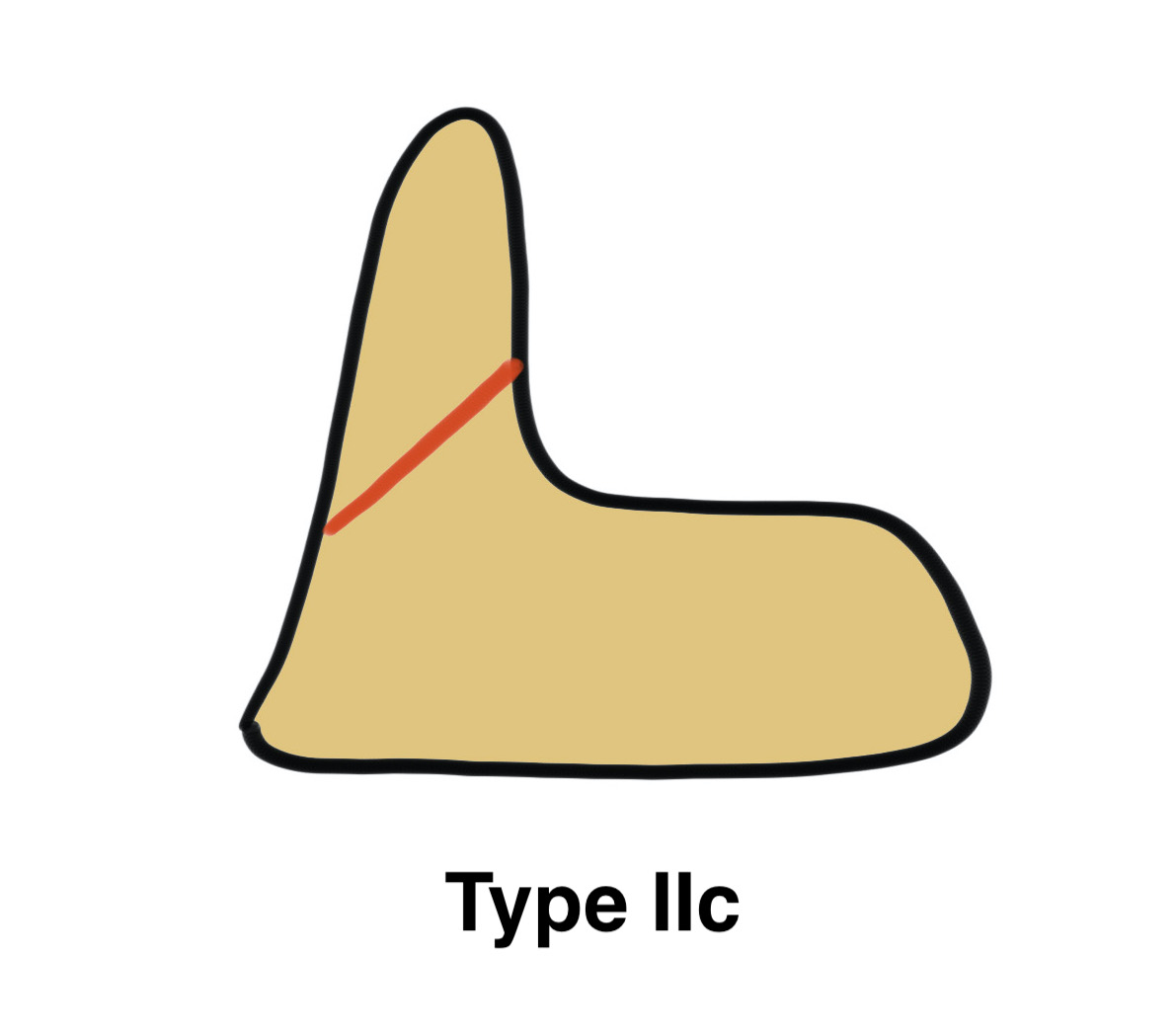
| Type IIIc |
Displaced Fracture line antero-inferior to posteror-superior Significant comminution |
No suitable for screw Posterior fixation / fusion |
Nonoperative Management
Indications
Minimally displaced
? Elderly


Collar versus Halo-Thoracic Brace
Waqar et al World Neurosurg 2017
- systematic review of halo (60%) versus collar (40%) in 714 cases
- 80% type II
- similar union rates for type II fractures
- increased failure rates with collar for type III fractures
- higher complications rates with halo vest
Operative versus nonoperative
Aldrian et al Neurosurgery 2012
- anterior screw fixation (25) versus halo vest (21)
- average age 64 years
- no difference in clinical outcome between groups
- nonunion rate 13% with screw
- nonunion rate 30% with halo vest
Operative management
Indications
Displaced
Operative Options
1. Odontoid screw
2. C1/2 fusion
- Brook's interlaminar wire
- C1 lateral mass / C2 pedicle screws (Goel Harms)
- Mageryl transarticular screws

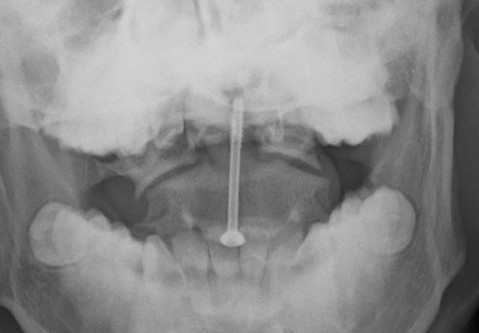
Odontoid screw

C1 lateral mass / C2 pedicle screw (Goel Harms)

Transarticular / Magerl screws from: Koepke et al Nature Reports
Results
- meta-analysis of odontoid screw versus posterior C1/C2 fusion
- overall increased union rate with posterior fusion
- most evident > 60 years of age
- no difference < 60 years of age
Ondontoid Screw Fixation
Advantages
Preserves C1/C2 cervical rotation compared to C1/2 fixation
Contra-indications
Irreducible fracture
- > 6 mm displacement
- > 10 degrees angulation
- fracture gap > 2 mm
Comminution or anterior oblique fracture configuration (Grauer Type IIc)
Poor bone stock
Pathological fractures
Odontoid + transverse ligament injury - will remain unstable
Body habitus - short neck
Anterior Odontoid Screw Technique

AO Foundation Surgical Technique
Skull traction
Image intensifier
Smith-Robertson approach
Identify antero-inferior margin of C2
Results
- ondontoid screw fixation in 102 patients
- nonunion rate 4% in patients < 65 years
- nonunion rate 10% in patients > 65 years
- systematic review of odontoid screws
- 5% malposition
- 5% screw cut out
- 3% screw fracture rate
- nonunion 10%
Complications
Dysphagia
Difficulty swallowing
Recurrent laryngeal nerve - vocal cord paralysis
C1/C2 fixation
Indications
Displaced fracture
Comminution / Poor bone
? Elderly
Unstable fracture configurations
Technique
Vumedi C1/C2 fixation for Type II dens fracture
Vumedi C1/C2 Goel and Harms technique
AO Surgery Reference C1/C2 fusion
Results
- 77 cases type II treated with C1/C2 posterior (screw/rod) fixation
- union rate 95% on CT
Elderly
Issue
Most common fracture of the cervical spine in the elderly
High risk of non-union
High risk of mortality
High risk of halo-thoracic brace
High risk of failure of fixation due to poor bone
Mortality
Allia et al Orthop Traumatol Surg Res 2020
- 79 patients mean age 85
- 3 month mortality 27%, 1 year mortality 30%
- 3 month mortality 11% in undisplaced fractures
- 3 month mortality 40% in displaced fractures
Operative versus nonoperative
Schroeder et al Neurosurgery 2015
- 1233 patients > 60 year old with type II odontoid fracture
- short and long term mortality lower with operative versus nonoperative treatment
- operative versus non operative treatment 1098 patients > 65
- no difference in short term mortality
- small difference in long term mortality favoring operative treatment
Nonunion
Issues
Pain
Instability / myelopathy
Risk sudden death
Types
Non union - unstable on flexion extension views
Fibrous nonunion - stable on flexion / extension views
Fibrous union
Florman et al World Neurosurgery 2022
- systematic review of 141 patients with fibrous nonunion / stable nonunion
- no neurological events
- neck disability ranged from mild to severe
- good to excellent pain scores
Nonunion / unstable




Significant instability on flexion / extension views after Type II odontoid nonunion
Options
C1/2 fusion

Type III
Definition
Through the body of C2
May involve portions of C1 or C2 facets
High healing potential
Non operative management
- 212 patients with Type III dens fracture
- average age 72, 20% lived independently
- 95% treated nonoperatively
- 5% required surgery
- 25 patients with Type III dens fracture
- hard collar or halo vest
- 22/25 (88%) united
- nonunion associated with increased coronal tilt and lateral mass gap > 2mm