Look
Splints
Extend elbow to side
- medial wounds
- extension
Flex elbow to side
- flexion range
Flex elbow to front
- olecranon wound
Extend elbow to front
- anterior wounds
- carrying angle
- forearm wasting
Palm up
- clawing
- hypothenar eminence
- scars

Thumb up
- thenar eminence

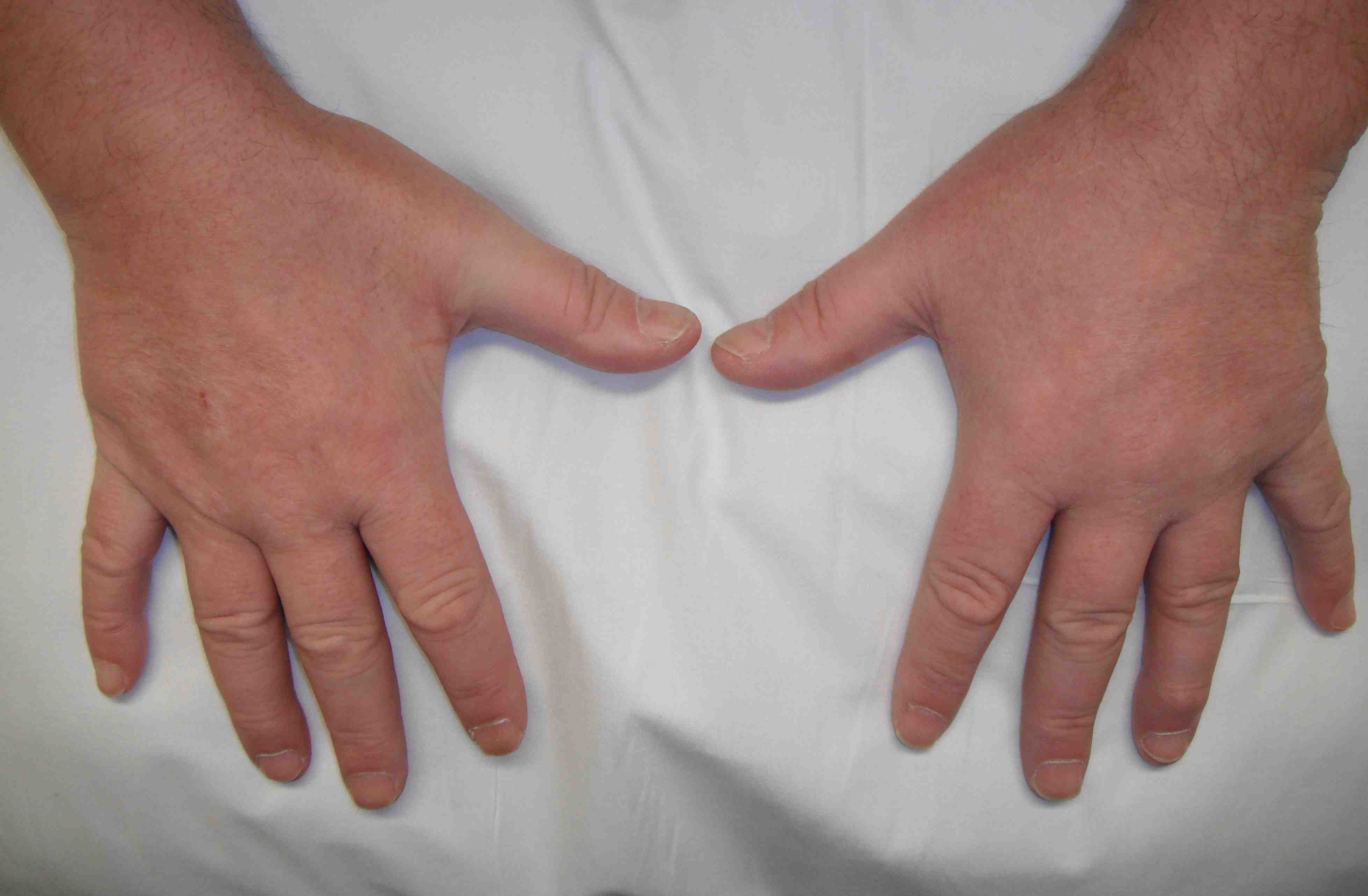
Palm down
- interossei / adductor pollicis wasting

Palms together
- claw
- hypothenar eminence
Feel
Sensation
1. LF & RF
2. Dorsal branch ulna nerve
- branches above wrist
- runs under FCU
- dorsum of hand, ulna side
- dorsum LF and half RF to P2
3. Palmar cutaneous branch
- above wrist
- hypothenar eminence
3. Medial forearm (MCNF / T1)
- above ulna
Move
Above elbow
1. FCU (C7)
- patient flexes wrist, palpate
2. FDP (C8)
- patient makes fist & resists extension of LF
Below wrist
1. AbDM
- LF together
- first branch deep nerve
2. 1st Dorsal Interossei
- push both IF together
- last branch deep nerve
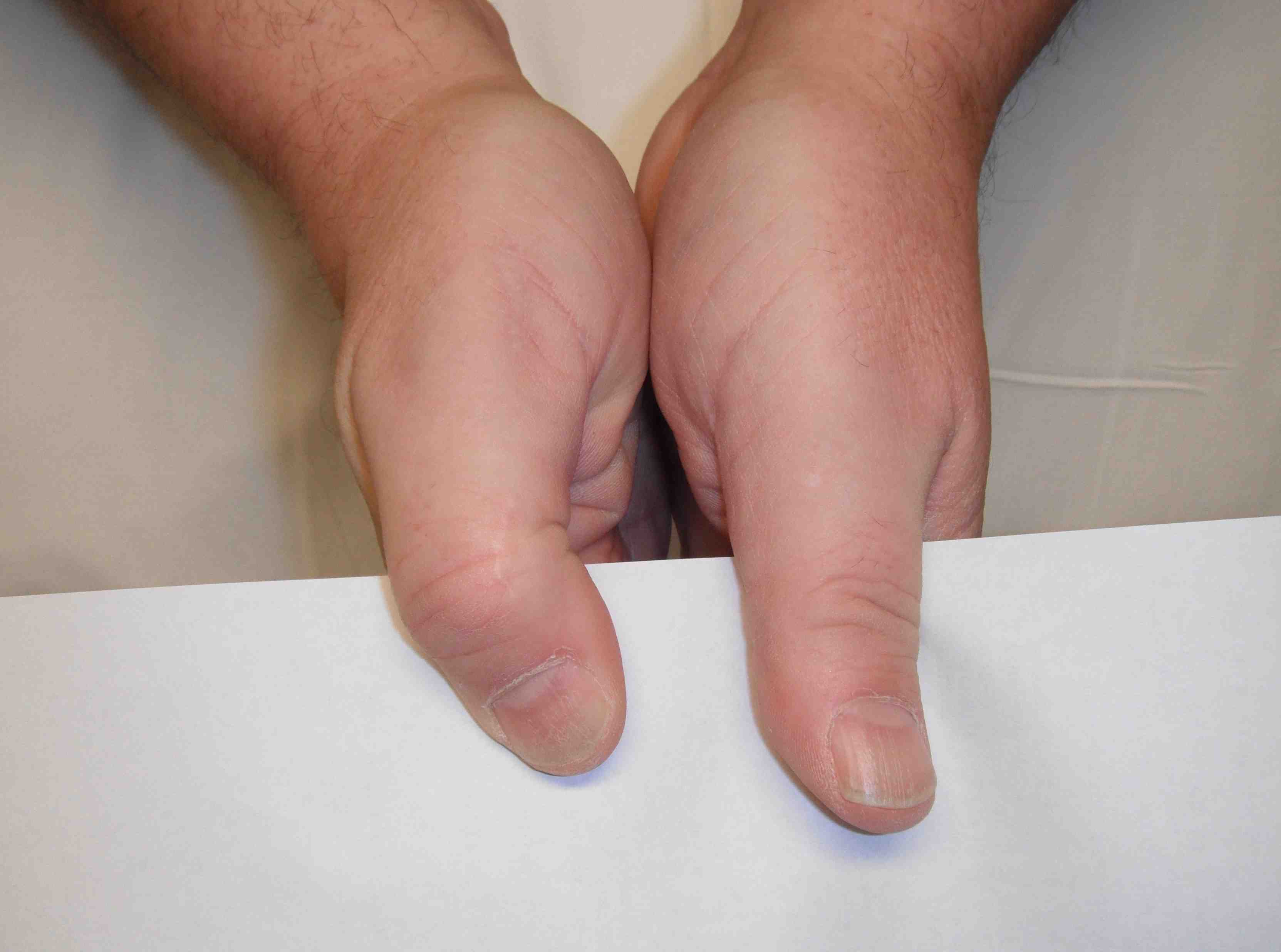
3. Adductor Pollicis
- Froment's sign
- hold paper between thumb and IF
- positive if patient uses FPL to grip
4. Card sign
- between index and middle finger
- PAD
- palmar interossei adducting
5. Lateral 2 lumbricals
- unable to pad to pad LF / RF
- lumbricals extend DIPJ
- patient can only tip to tip
Special Tests
Tinel's - Cubital tunnel, Guyon's
Ulna nerve subluxation / tenderness
DDx
T1
- thumb APB weak / wasted
C8
- EDC / Wrist extension weak
TOS
- sensory loss above wrist
- Addson sign
Compression Syndromes
1. Medial Intermuscular septum
- arcade of Struthers (fascial band)
- septum
- hypertrophied medial head triceps
2. Medial epicondyle
- tardy ulna nerve palsy, previous fracture
3. Epicondylar groove
- intrinsic (SOL, synovitis, rheumatoid nodule
4. Cubital Tunnel
- tendinous arch of FCU
5. Exit FCU
6. Guyon's canal
- FDP OK
- palmar & dorsal br spared
- all small hand m's affected
7. Deep motor branch only
- can be compressed against pisiform & hamate
- with using mallet, vibrating tools
- sensation normal