Arthroplasty
Indications
Patient > 70
Gjertsen et al JBJS Am 2010
- 4335 patients > 70 with displaced subcapital fractures
- minimum 1 year follow up
- 1 year mortality same in each group / 25%
- 22% reoperation in ORIF v 3% in hemiarthroplasty
- more pain / higher dissatisfaction / lower quality life in ORIF group
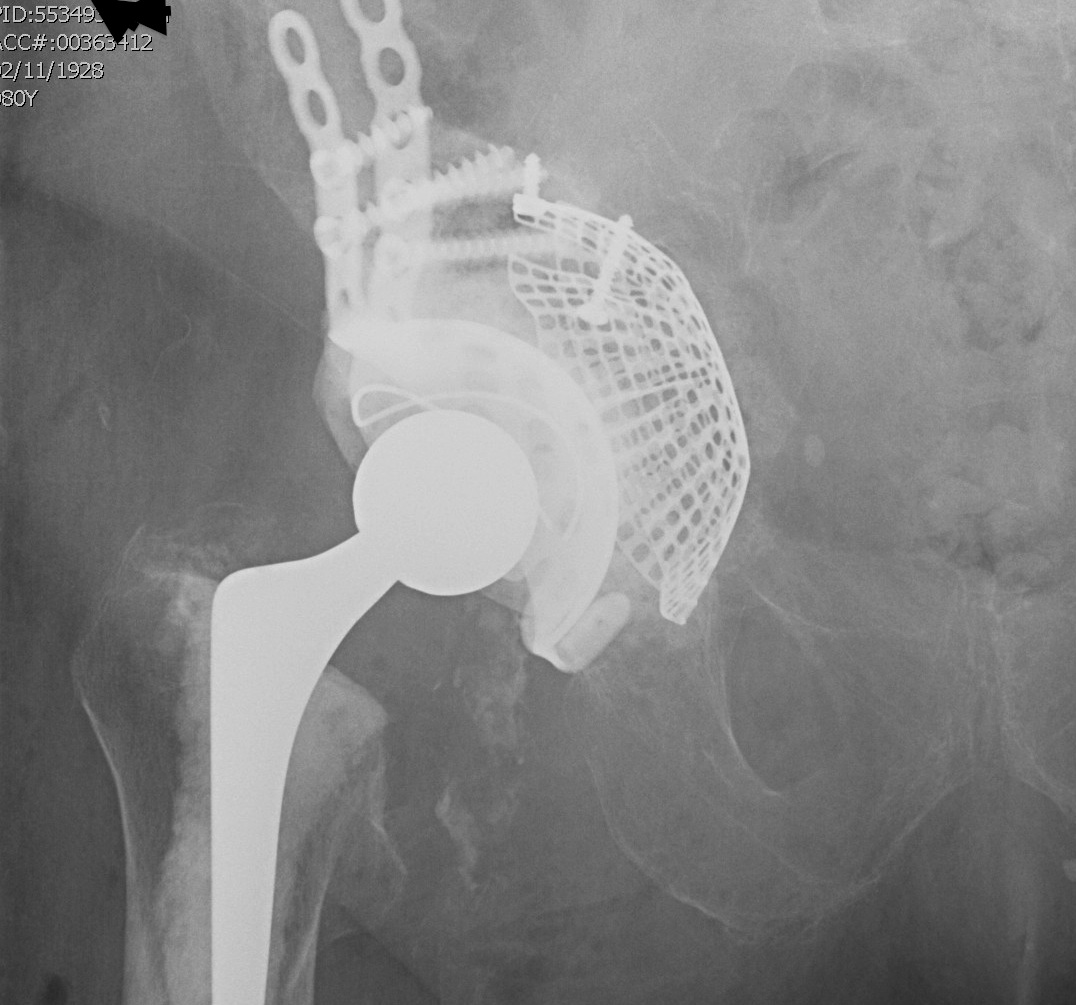
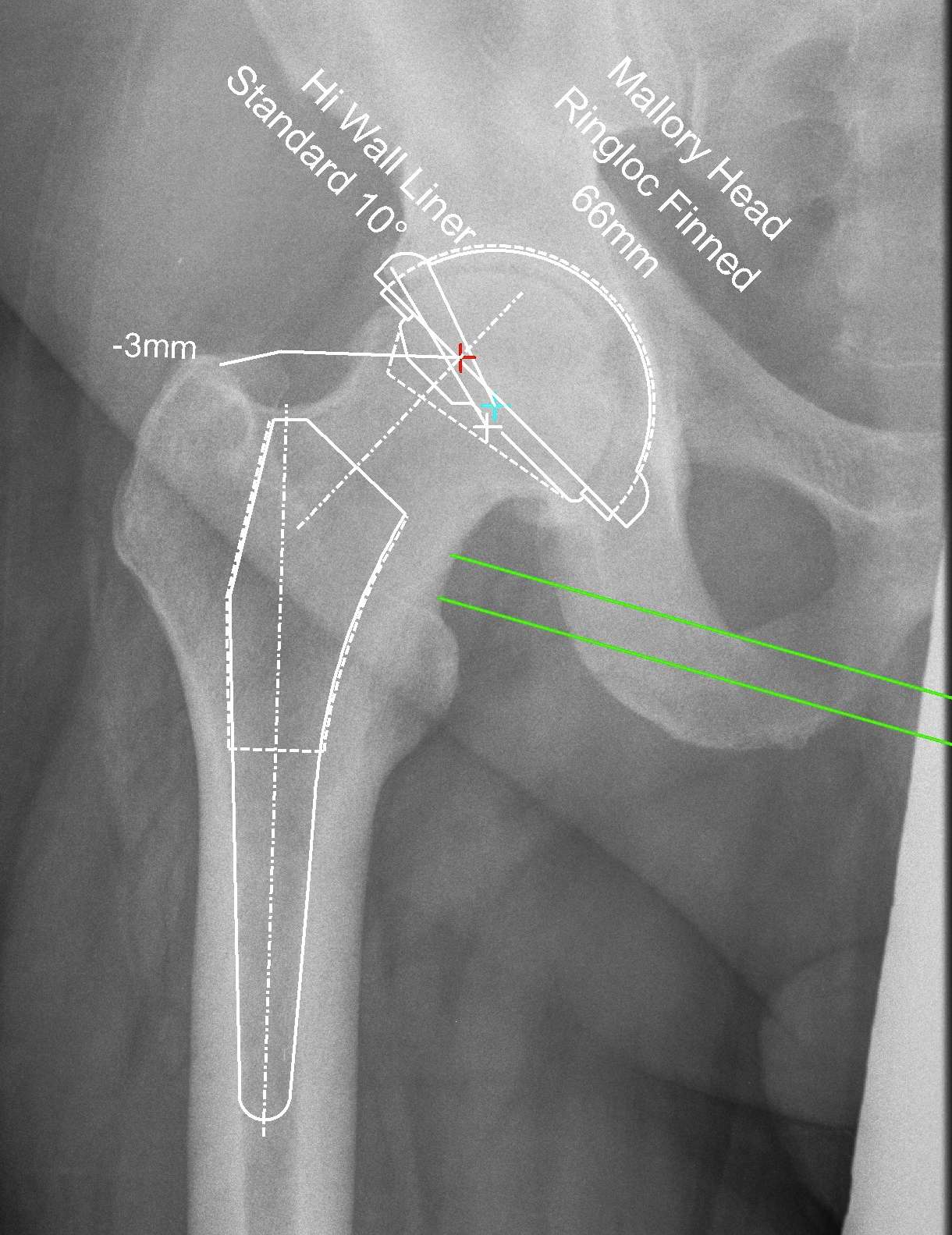
Options
Hemiarthroplasty
- unipolar monoblock
- unipolar modular