Definition
Painful impingement of rotator cuff
- on anterior 1/3 of Acromion, CA ligament & ACJ
- causes tendinosis of the RC
Anatomy Subacromial Space
1. Roof / CA Arch
- acromion
- CA ligament
- coracoid process
- ACJ is superior & posterior to CA ligament
2. Floor
- GT & superior aspect head
- rotator cuff
Aetiology
Controversial
- extrinsic and intrinsic theories
1. Extrinsic / Extra-tendinous / Bursal sided tears
CA arch impinges on RC
- true impingement syndrome
- causes tendinosis of the cuff
Factors
A. Subtle GH Instability
- relationship poorly understood
- respond poorly to acromioplasty
- alteration in dynamics of shoulder
B. Internal Impingement Posterior / Superior Glenoid
Described by Davidson 1997
- throwing athletes
- impinge in abduction & ER
- SS impinges on posterosuperior rim of glenoid
- normally humeral head translates posterior in glenoid
- this may be lost with instability or laxity of throwing athlete
- alternatively may be caused by posterior capsular tightness
See Miscellaneous/Throwing Athlete
C. Degeneration ACJ
OA Spurs
D. Acromion Morphology
Neer = impingement on anteroinferior acromion
E. Os Acromiale
- mesoacromion most common
- hypermobile unfused epiphysis
- tilts anteriorly
- 1-15% normal population
- increased incidence with impingement
F. CA Ligament Spurs
Develop calcium in tendon
G. CA Ligament Impingement
- common
- "Snapping shoulder"
- in flexion & IR
- SS & Biceps impinge on it
- Neer recommends division
H. Coracoid Impingement
- less common
- subscapularis impingement between coracoid and LT
- may be exacerbated by anterior instability
- more medial pain with arm flexed, adducted and IR
- find SSC partial tears on arthroscopy

2. Intrinsic / Intra-tendinous / Articular sided tears
2° to bursal thickening or intrinsic problem in cuff
- ? Now thought to be most common
Factors
1. Muscle Fatigue
- overloaded weak muscles
- eccentric tension load
- associated with proximal humeral migration
2. Shoulder Overuse
- soft tissue inflammation
- repetitive microtrauma
- athletes / manual labourers
3. Degenerative Tendinopathy
- 1° intrinsic degeneration of RC
- ? hypovascularity
- increasing incidence with age
Pathology
Impingement Zone
- centered on supraspinatus tendon insertion
- Codman's "Critical Zone" 1cm from insertion
- zone of hypoperfusion
Neer's Pathological Classification
Stage I
- reversible
- oedema & haemorrhage
- < 25 years
Stage II
- irreversible change
- fibrosis & tendinitis
- 25-40 years
Subdivided by Gartsman
- Stage IIA = No tear
- Stage IIB = Partial thickness tears
Stage III
- > 40 years
- chronic
- partial & full thickness tears
Acromial Morphology
Bigliani / Assess on Supraspinatous Outlet View / Scapula Lateral
Type I: Flat
- 20% of normal population
Type II: Curved
- 40% of normal population

Type III: Hooked
- 40% of normal population
- 80% of RC tears



Cadaver study
- 30% of all cadavers had a full thickness cuff tear
- 75% type III & 25% type II & 3% type I
Morphology does change with age
- Spur more common > 50 years
- ? 2° event to cuff process
- most hooks appear to be acquired & lie in CA ligament
Symptoms
Painful arc
Weakness overhead
If < 40 years look for instability
Examination
Painful Arc
- 70-120°
- > 120° - ACJ OA / terminal phase pain
IR
- limitation of IR may suggest posterior capsular tightness
Neer Impingement Sign
- stabilize scapula from behind patient
- passively elevate arm in scapula plane
- pain between 70-120°
Hawkins Modification
- IR humerus at 90° flex
Neer Impingement Test
- LA in SAD
- abolish pain & test for cuff tear / weakness
Always
- anterior apprehension / Jobes relocation (young patient)
- ACJ assessment
- biceps assessment
- NVI
- C spine
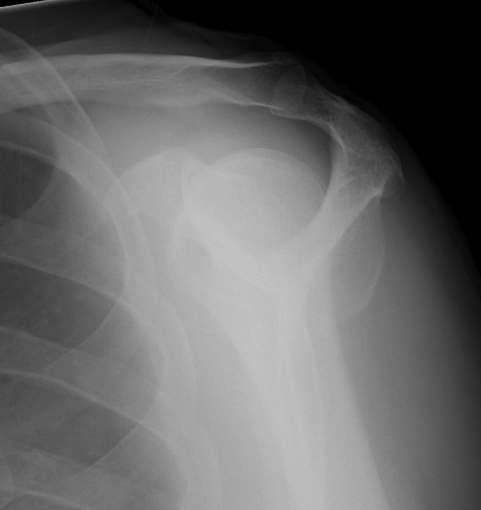
X-ray
AP view (True AP)
- acromio-humeral interval: Normal 1-1.5 cm, < 0.7cm abnormal
- sclerosis greater tuberosity / acromion
- lateral Acromion spur
- OA ACJ

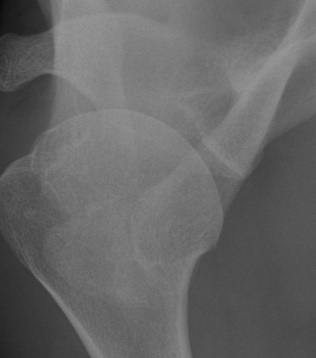
Axillary Lateral
- os acromion
- bone scan to exclude symptomatic hypermobility
Supraspinatus Outlet View
- Acromion morphology / calcification Coraco-Acromial Ligament
- scapula lateral variant
- plate on affected shoulder, other turned out of way
- 10° caudal
Zanca view
- ACJ
- half voltage / centred on ACJ / 10o cephalad
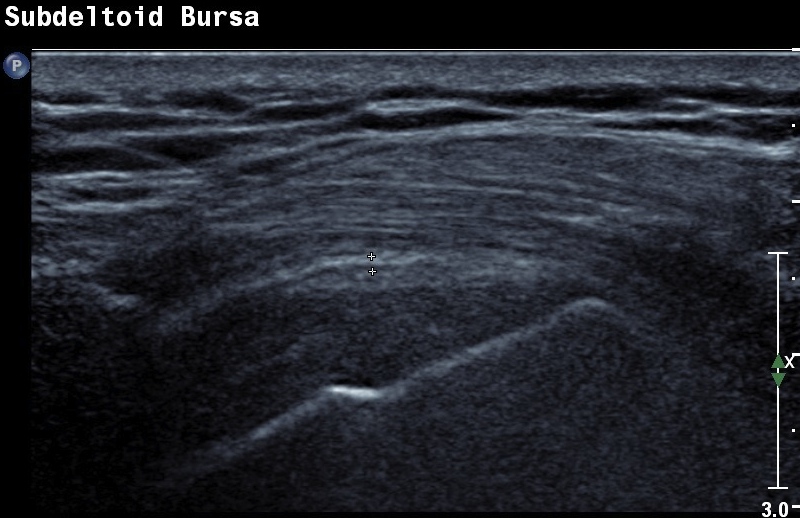
US
Diagnose
- dynamic impingement
- bursitis
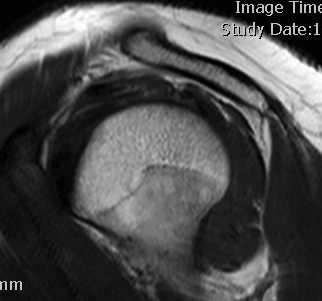
MRI
Sensitive
- assess acromial morphology
- look for tendinosis / tears
Management
Non Operative
HCLA injection
Goals
- decreases pain & inflammation
- diagnostic
Alvarez et al Am J Sports Med 2005
- RCT HCLA v LA in RC tendonosis
- no clinical difference between the two groups
Cuff Rehabilitation
Rockwood 3 Stages of Physio
1. Decrease Inflammation / Increase ROM
- rest
- gentle ROM
- posterior capsular stretches
- scapula & trunk stabilisers
- modify activities
- NSAIDS
2. Cuff Stabilisation and Balancing
- strengthen humeral depressors
- work on SSC and IS
- takes load off SS
- theraband / IR / ER exercises
- avoid abduction drills
3. Deltoid strengthening
- task specific exercises
Operative Management
Acromioplasty
Theory
Believe primary problem is extrinsic impingement
- abnormal acromial morphology on outlet view
- spurs in CA ligament
Results
Ketola et al JBJS Br 2009
- RCT of patients with impingement
- treated with exercise program or acromioplasty + exercise program
- no difference between the two groups
Henkus et al JBJS Br 2009
- RCT of bursectomy alone v bursectomy + acromioplasty
- no difference between the two groups
Open v Arthroscopic Acromioplasty
Results
Sachhs JBJS 1997
- open v arthroscopic
- open longer return to work & in hospital stay
- results similar
Davis et al Am J Sports Med 2010
- meta-analysis of open v arthroscopic acromioplasty
- no significant difference in outcome
- longer return to work and inpatient stays