Background
Anatomy
Pelvis is a true ring
- any anterior fracture must have a posterior injury as well
- integrity of the posterior sacroiliac complex is key
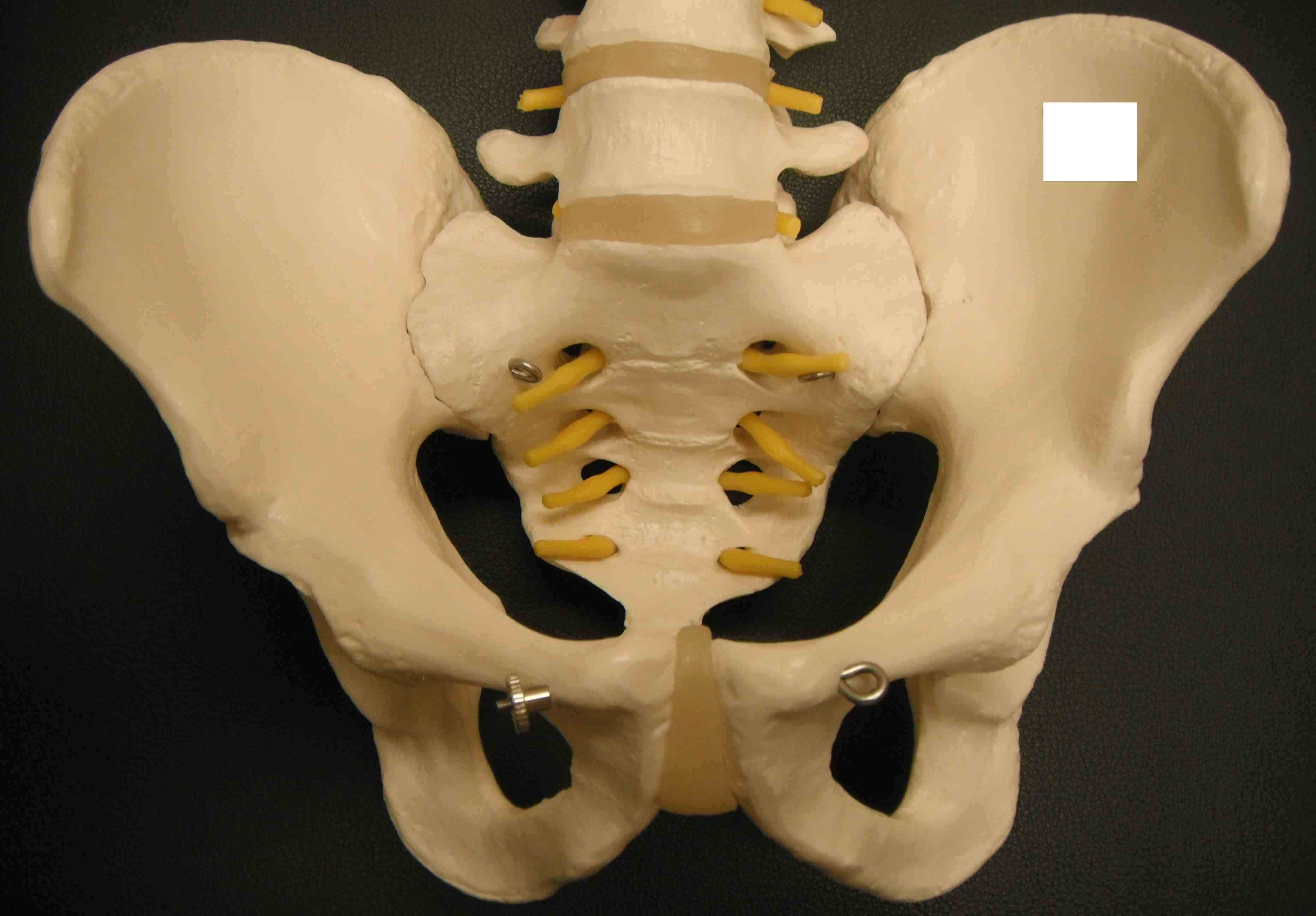
Bony Anatomy
2 innominate bones + sacrum
Symphysis pubis < 5mm
SI joint 2-4 mm
Pelvis is a true ring
- any anterior fracture must have a posterior injury as well
- integrity of the posterior sacroiliac complex is key
2 innominate bones + sacrum
Symphysis pubis < 5mm
SI joint 2-4 mm
Irradiate a slice of tissue from multiple angles
Measure the output from different sides
Tissues have different densities
- with denser tissue fewer x-rays reach the detectors
Bone 2000
ST 40
Water 0
Fat -100
Air -1000
Patella may develop from one or multiple ossification centres at 3 years
Failure of centres to fuse may produce bipartite or tripartite patella
- usually bilateral and painless
Classically superolateral
I Inferior Pole 5%
II Lateral 20%
Quantify Valgus Malalignment


30o flexion

Non-traumatic or traumatic condition of femoral head with bone death
20 - 50 yo (average 38)
- M: F 4:1
70-80% with AVN will progress within 1 year
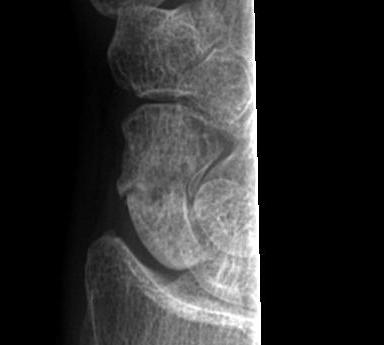
Young men
FOOSH
- axial load, dorsiflexion and radial deviation
DISI occurs in ulna deviation
Type A Stable acute fracture
A1 Tubercle

Convincing association with development of osteoarthritis
- arthritic changes beginning at radial styloid
- progress to scaphocapitate & capitolunate

Extremely uncommon
Stability provided by joint capsule /costoclavicular & interclavicular ligaments
Recurrent instability uncommon
Many apparent dislocations in adolescents may be growth plate injuries
-will remodel without treatment
If OA from chronic dislocation may resect SCJ
Patients usually complain of subluxation rather than dislocation
- rarely requires reduction
Different entity to acute posterior dislocation usually
Rare
1. Ligamentous laxity > 50%
- commonly associated with MDI
- posterior only 20%
- posterior & inferior 20%
Rare
- 2% of acute dislocations
Often missed
- < 1/ 52 25%
- < 6/52 25%
- < 6/12 25%
- > 6/12 25%